

Shoulder pain when lifting the arm is typically caused by rotator cuff tendinopathy or subacromial bursitis, affecting roughly 2.4% of primary care patients annually.
These conditions result from mechanical irritation or overloaded tendons, most of which recover within 6–12 weeks through targeted strengthening and load management.
If you’re dealing with shoulder pain when lifting your arm, you’re not crazy, and you’re definitely not alone. 2.4% of people in the UK primary care seek help for shoulder pain each year.
Now, as athletes, we feel everything in our shoulders. They’re involved in almost every lift, strike, grip, and scramble. When something feels off, it messes with more than just training; it messes with your confidence.
The good news? Most cases aren’t catastrophic tears or career-ending injuries. They’re irritated, overloaded tissues asking for smarter management.
This 2026 clinical guide explores:
-
What causes the "painful arc" during overhead lifts?
-
How do you distinguish between bursitis and a rotator cuff tear?
-
When are red flags indicative of emergency medical needs?
-
Which rehabilitation strategies offer the highest ROI for athletes?
And if you need support while you recover, our Anaconda Shoulder Brace is designed to stabilize, protect, and help you train with confidence, without locking you up as bulky braces do.
Key Takeaways
-
That sharp or pinching pain when you raise your arm is incredibly common. Most of the time, it’s irritated tendons or bursa in a tight space above the shoulder — not a full tear or something permanently damaged.
-
You can narrow down the likely issue fast by noticing patterns: where the pain shows up (front, side, or top), when it hurts most (on the way up or lowering down), and whether stiffness or pain is what’s really limiting you.
-
The majority of people improve within 6–12 weeks just by adjusting aggravating movements and doing focused strengthening work. MRIs aren’t usually needed early on unless symptoms persist past 12 weeks.
-
Red flags matter. If you suddenly can’t lift your arm at all, feel severe pain or weakness after an injury, notice visible deformity, have swelling with fever, or experience chest pressure along with shoulder pain — that’s medical-attention-now territory.
-
A simple 7–10 day reset, such as avoiding your biggest aggravators, keeping gentle movement, and gradually adding low-load exercises, can shift momentum in your favor. Knowing when to push and when to escalate gives you control instead of fear.
Why That “Pinch” Happens Mid-Lift (And Why It Feels So Sharp)
You know the exact moment.
Your arm gets halfway up, not at your side, not fully overhead, but right in that middle zone. Then it catches. Sharp. Annoying. Sometimes it even feels weak or unstable.
Here’s what’s happening inside, in simple terms.
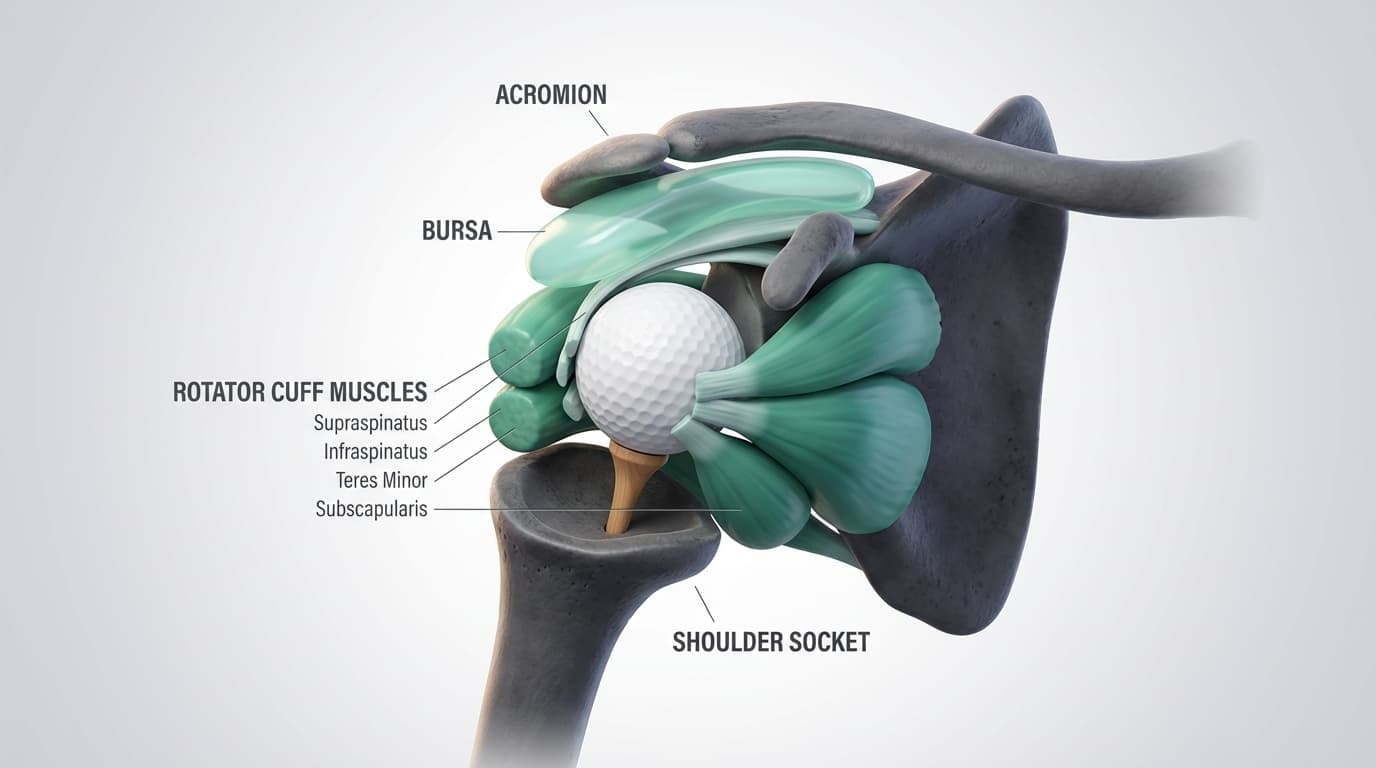
The anatomy of your shoulder is basically a golf ball sitting on a tee. The ball (your upper arm bone) rests in a shallow socket on your shoulder blade.
The shoulder joint is designed for mobility first and stability second. This high range of motion allows athletes to punch, press, and swim, but relies on the rotator cuff for active stabilization during load.
Holding that ball centered are four key shoulder muscles called the rotator cuff. Above those tendons sits a small fluid-filled cushion called the bursa. Its job is to reduce friction as everything glides under the bony roof of your shoulder (the acromion).
When everything is balanced, the ball stays centered, the tendons glide smoothly, and movement feels effortless.
But when training volume spikes, posture shifts, recovery dips, or the biomechanics of the shoulder get sloppy, the ball can ride slightly upward during a lift. That narrows the space above it, and the tendons and bursa don’t love that.
So when you lift your arm, especially between about shoulder height and overhead, those irritated tissues can get compressed. That’s the “pinch.” That’s the catch. That’s the sharp reminder.
And here’s something reassuring. Imaging studies show that many people with no pain have partial tears or tendon changes on scans. Therefore, structure doesn’t always equal symptoms. To fully diagnose shoulder impingement syndrome, medical professionals identify signs of irritation and load tolerance, not destruction.
That’s why most shoulder pain when lifting arms improves with smart load management and strengthening, not surgery.
The key is understanding whether your shoulder just needs recalibration… or whether it’s waving a bigger red flag.
60-Second Shoulder Reality Check (Before You Panic)
When athletes feel shoulder pain when lifting their arm, the brain goes straight to the worst-case scenario.
Tear…
Surgery….
Months off.
We get it. But here’s the truth: most shoulder pain patterns are predictable. And if you can identify the pattern, you can usually manage it intelligently.
This self-check isn’t about pushing through pain. It’s about observing and identifing it.
Move slowly. Stay below sharp, stabbing pain because you’re gathering information, not testing your toughness.
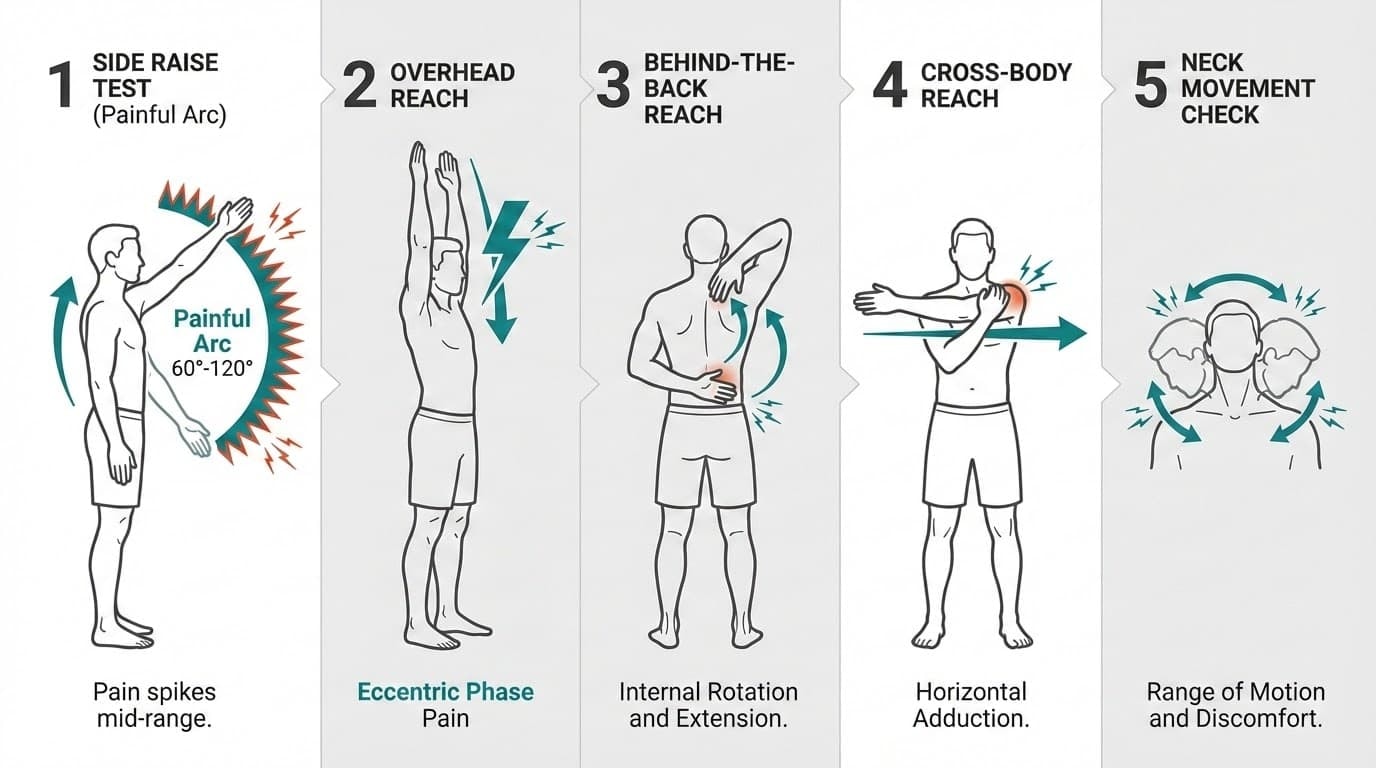
1. The Side Raise Test (Painful Arc)
For the painful arc test, first you have to stand tall. Lift your arm straight out to the side like you’re making a snow angel.
If pain spikes between shoulder height and just above (roughly mid-range or 60 to 120 degrees), that usually points toward rotator cuff problems or subacromial irritation.
If it only hurts at the very top, or not in the middle at all, that suggests a different structure.
That mid-range “catch” is classic for overloaded cuff tendons or irritated bursa.
2. The Overhead Reach
Reach up like you’re grabbing something off a high shelf. What do you notice?
Is it worse going up? Or worse, lowering back down?
Pain during lowering (the eccentric phase) is common with tendinopathy. That controlled descent loads the tendon more, and irritated tendons complain.
3. Behind-the-Back Reach
Reach behind your back like you’re tucking in a shirt.
If it hurts, but you can still move, that’s one thing. If it feels like you hit a hard wall of stiffness no matter what, that leans toward a frozen shoulder pattern.
4. Cross-Body Reach
Bring your arm across your chest like you’re putting on a seatbelt.
Sharp pain right on top of the shoulder where the collarbone meets it? That raises suspicion for AC joint irritation. Research shows this test has about 77% sensitivity and 79% specificity for chronic AC joint problems.
5. Quick Neck Check
Turn your head side to side. Tilt your ear to your shoulder.
If that reproduces your “shoulder” pain, especially with tingling or burning down the arm, your neck may be involved.
Quick Pattern Cheat Sheet
Now, to make it easier for you, here’s a quick cheat sheet:
-
Mid-arc side/front pain → likely rotator cuff or subacromial irritation
-
Top-of-shoulder pain with cross-body reach → possible AC joint involvement
-
Major stiffness in all directions → frozen shoulder pattern
-
Neck movement changes symptoms or causes tingling → possible cervical referral
Just remember that this doesn’t replace a proper exam by a trained medical professional. But it gives you clarity. And clarity reduces fear.
The Usual Suspects Behind Shoulder Pain When Lifting The Arm
Multiple structures can create similar pain patterns. That’s why jumping straight to an MRI often creates more confusion than answers.
Here are the most common patterns we see.
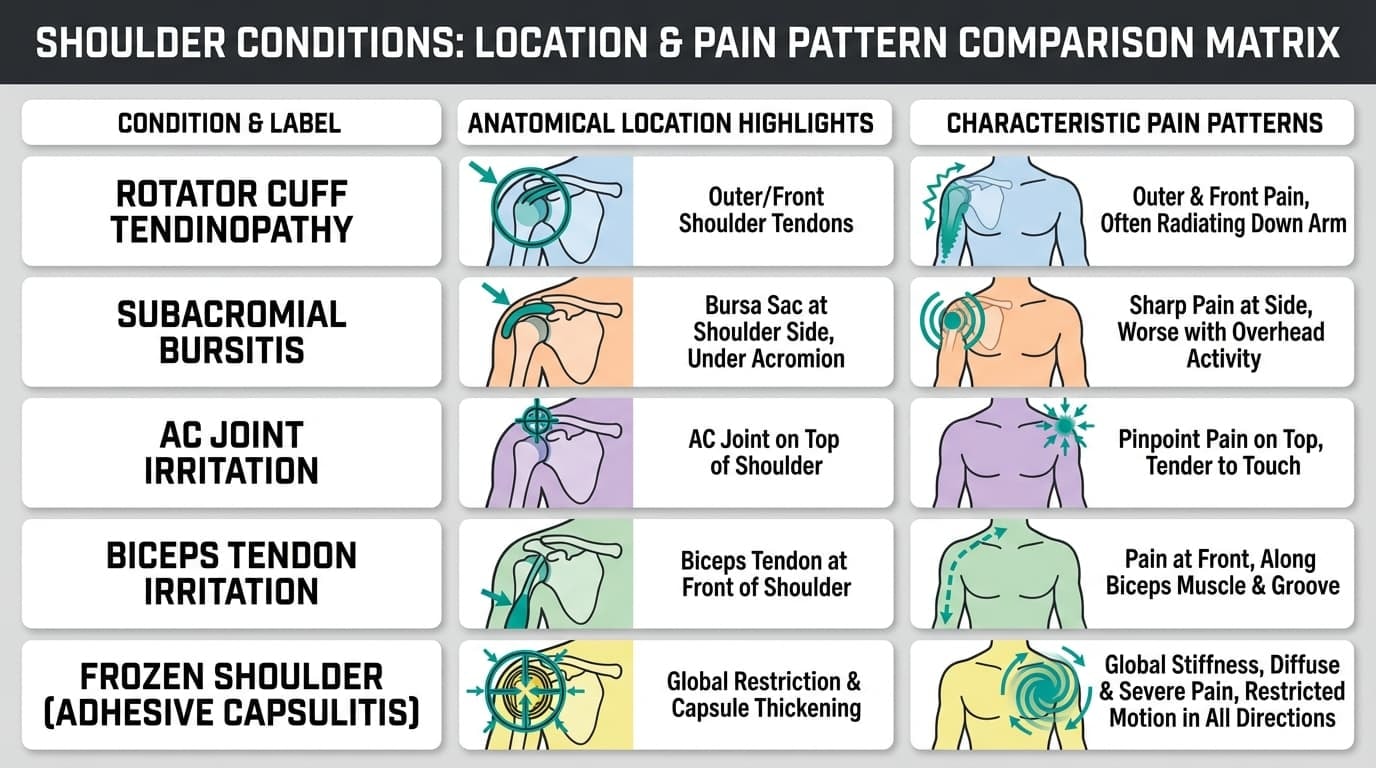
Rotator Cuff Tendinopathy (a.k.a. The Overloaded Stabilizers)
Rotator cuff tendinopathy is the heavyweight champ of shoulder pain when lifting the arm. With a rotator cuff injury, pain usually sits on the outer or front of the shoulder and hits hardest during that mid-range lift.
Common triggers:
-
Overhead pressing
-
Throwing
-
Swimming
-
Painting ceilings
-
Repetitive overhead work
-
Sleeping on that side
What’s happening? The rotator cuff tendons become irritated by repeated loading, poor shoulder blade control, or volume spikes. They’re overloaded, not necessarily torn.
Pain is often worse when lowering the arm than when raising it. Not to mention, nights can be annoying.
The good news is that most cases of rotator cuff tendinitis respond extremely well to load management, joint stabilization, and targeted strengthening.
Also, this is where supportive compression, like our Anaconda Shoulder Brace, can help during the return-to-training phase. It doesn’t “fix” the tendon. But stabilizing the joint and improving proprioceptive feedback can reduce strain while you rebuild capacity.
Support plus smart rehab beats rest alone.
Subacromial Bursitis (The Angry Cushion)
The bursa is a friction-reducing cushion above the rotator cuff. When it’s inflamed, it is called subacromial bursitis, and it mimics cuff pain:
-
Ache on the side of the shoulder
-
Sharp pain overhead
-
Pain lying on that side
Bursitis and cuff irritation often coexist. Treatment overlaps heavily, which is to modify load, improve mechanics, and gradually strengthen. Injections can sometimes temporarily relieve shoulder pain, but they don’t fix the underlying cause.
AC Joint Irritation (Top-of-Shoulder Pain)
AC joint irritation sits right on top of the shoulder.
You’ll usually feel:
-
Sharp pain directly on top
-
Pain when bringing the arm across the body
-
Discomfort with heavy bench, dips, or push-ups
Lifters and grapplers who’ve taken falls on the shoulder are especially prone.
Management often starts with reducing direct compression (temporarily backing off dips and heavy flat pressing) and strengthening the surrounding muscles.
Athletes who’ve taken falls directly onto the shoulder or who load heavy horizontal pressing frequently are at higher risk.
Treatment typically involves temporarily reducing compressive movements, strengthening surrounding musculature, and gradually reintroducing load.
Again, bracing with the Anaconda Shoulder Brace isn’t about masking pain. It’s about providing controlled stability while tissue tolerance rebuilds.
Biceps Tendon Irritation (Front-of-Shoulder Ache)
For biceps tendon irritation, pain is more localized to the front.
Worse with:
-
Heavy curls
-
Carrying weight in front
-
Straight-arm overhead movements
To test this condition, press into the groove at the front of your shoulder. If it’s tender there, this tendon may be involved.
The fix to reduce pain? Lessen provocative loads, strengthen the cuff and scapular stabilizers, and stop constantly “pushing” it.
Frozen Shoulder (When Everything Gets Tight)
Frozen shoulder goes beyond pain; it’s stiffness. It involves the capsule, which is the connective tissue around the shoulder joint, becoming stiff, thickened, and tight. Instead of just having painful spots in the arc of motion, you can experience global loss of motion in multiple directions.
You’ll notice:
-
Progressive loss of motion in multiple directions
-
Trouble reaching overhead, behind your head, or behind your back
-
A true hard stop in movement
Both active and passive motion are restricted.
It’s more common among people between 40 and 60 years old, those with diabetes or thyroid issues, or after long periods of not moving the arm at all, that is, complete immobilization. Also, it can take many months to fully resolve, but it usually improves over time.
Neck-Related Referral (It’s Not Always the Shoulder)
Sometimes the shoulder is innocent, and the pain is coming from the neck. The nerves exiting the cervical spine can refer pain to the shoulder blade, the outer shoulder, or down the arm, mimicking shoulder problems.
In fact, large studies show that scapular (shoulder blade) pain pops up in about 72% of people with cervical nerve root irritation.
Clues:
-
Neck stiffness
-
Tingling or burning down the arm
-
Symptoms that change when you move your neck
True shoulder irritation usually stays local. Nerve-related pain often radiates.
However, if you notice weakness, numbness, changes in hand coordination, or ongoing neurological symptoms, that’s not DIY territory. Get assessed by your doctor immediately!
The Line Between Smart Self-Care and Risk
At Anaconda, we believe in training smart, not training scared.
Most shoulder pain when lifting the arm improves with:
-
Temporary load modification
-
Gradual strengthening
-
Controlled mobility
-
Joint stabilization during return to sport
Our Anaconda Shoulder Brace was built for that middle ground, the phase where you’re rebuilding strength but still need support. With 3D compression and optional gel padding for impact protection, it stabilizes without restricting the range of motion.
But here’s the important part:
A brace is a support tool, not a substitute for proper assessment when red flags are present.
We’ve lived through major injuries. We understand the fear of setbacks. Our promise is simple: help you protect your body so you can keep doing what you love, safely, confidently, and long term.
When Shoulder Pain Is Just Annoying… and When It’s a Red Flag
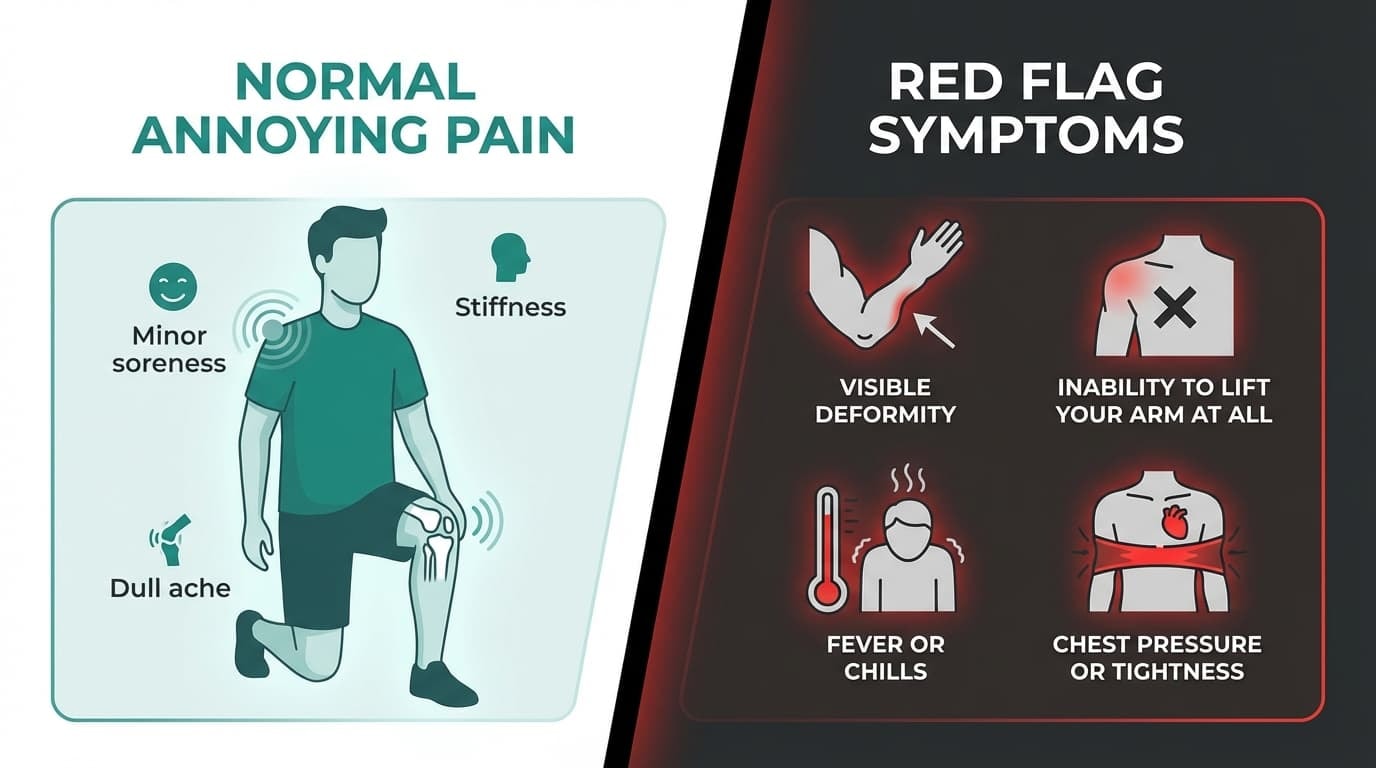
Most cases of shoulder pain when lifting the arm fall into the “irritated but safe” category.
It hurts. It’s frustrating. It might mess with your sleep or your training. But it’s slowly improving; you can still move it, and nothing feels dramatically unstable or weak.
That’s usually tendon or bursa irritation. Uncomfortable, yes. Dangerous? Rarely.
But there are moments when shoulder pain is not something to push through.
Trauma-Related Red Flags
If your pain started after a fall, collision, or heavy lift and you felt a pop followed by immediate weakness or loss of motion, that’s different.
Watch for:
-
Visible deformity
-
Shoulder looking “out of place”
-
Inability to lift your arm at all
-
Sudden, severe weakness
If you can’t actively lift your arm after trauma, don’t self-rehab it.
Get evaluated by your doctor ASAP!
Systemic Warning Signs
These are rare, but still important.
Seek urgent care if shoulder pain comes with:
-
Fever or chills
-
Redness, warmth, or major swelling
-
Unexplained weight loss
-
History of cancer
-
Multiple swollen joints
That’s not typical overuse pain. That’s medical territory.
Cardiovascular Symptoms (Do Not Ignore)
If shoulder pain is accompanied by:
-
Chest pressure or tightness
-
Jaw or left arm pain
-
Shortness of breath
-
Unexplained sweating
That’s not orthopedic. That’s emergency care. Call for medical help.
Time-Based Concerns
Even without red flags, pay attention to the timeline.
If you’re experiencing shoulder pain when lifting your arm that:
-
Isn’t improving at all after 2–3 weeks of smart load modification
-
Is getting worse instead of plateauing
-
Wakes you every single night, despite position changes
-
Causes progressive weakness
It’s time for a medical review.
Getting help doesn’t show weakness. It protects your longevity.
How Shoulder Pain Gets Diagnosed (Without Jumping Straight to an MRI)
Here’s something most people don’t realize:
You usually don’t need a scan right away.
Shoulder pain when lifting the arm is typically diagnosed clinically, meaning through history and physical examination.
A good clinician will ask:
-
Where exactly is the pain?
-
Did it start suddenly or build gradually?
-
What movements trigger it?
-
Does it affect sleep?
-
Any prior shoulder or neck issues?
Then they’ll examine:
-
Active vs. passive range of motion
-
Rotator cuff strength in multiple positions
-
Painful arc testing
-
Cross-body AC joint testing
-
A basic neck screen
Imaging is usually reserved for:
-
Suspected large full-thickness tears of rotator cuff muscles
-
Persistent symptoms beyond 6–12 weeks
-
Atypical or worsening cases
-
Surgical consideration
Why?
Because imaging often shows “abnormalities” in people with zero pain. A tendon can look irritated on MRI and still be functioning fine. And a normal scan doesn’t mean your pain isn’t real.
Symptoms and function matter more than pictures to treat shoulder pain.
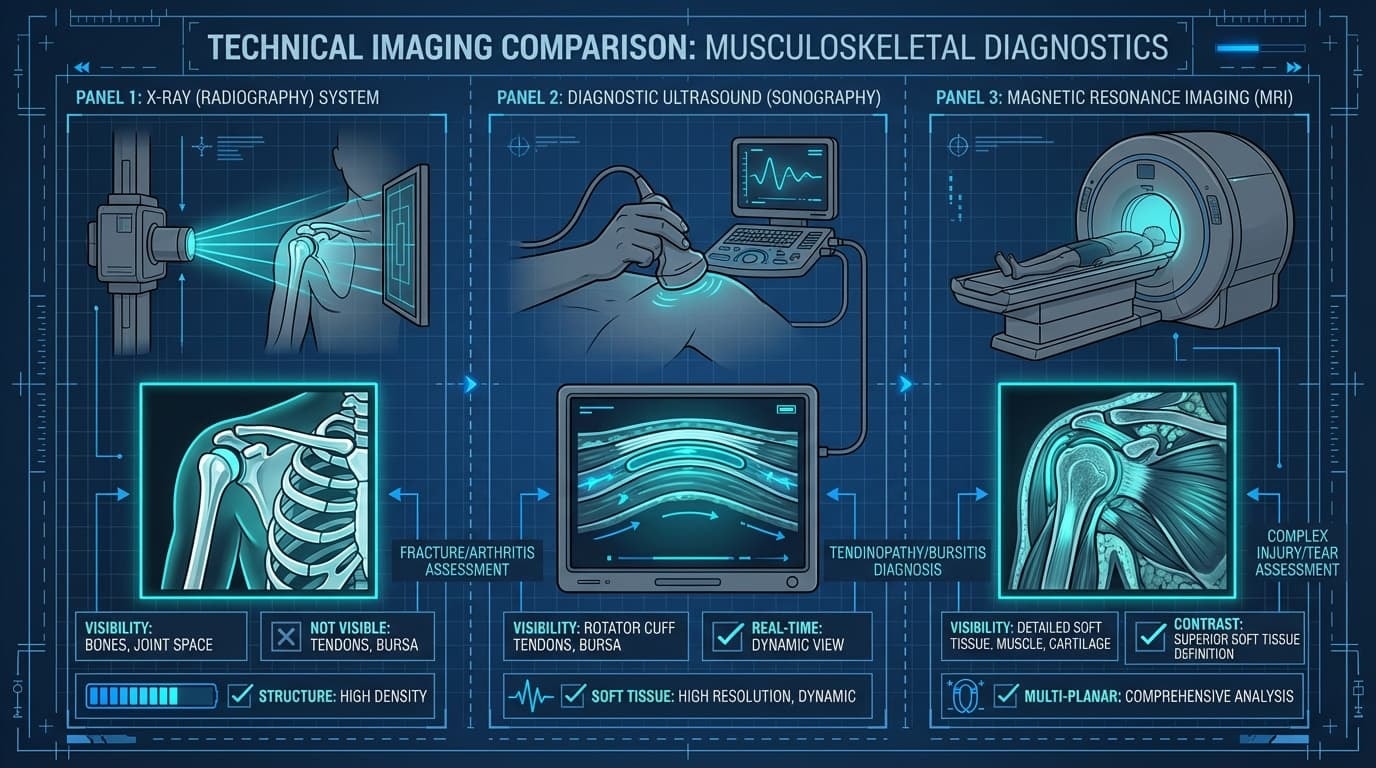
X-Ray, Ultrasound, or MRI? What They Actually Show
Let’s simplify this.
X-Ray
An X-ray shows the bones and joint space of the shoulder. Plus, it is helpful for identifying fractures, more advanced arthritis, or bone spurs.
If there has been trauma or there is concern about a structural bone issue, this is often the first imaging test ordered. However, X-rays do NOT clearly show tendons or the bursa, so they are not very useful for most soft-tissue shoulder problems.
Ultrasound
Ultrasound allows us to see the rotator cuff tendons and the bursa. One major advantage is that it can assess movement in real time, meaning we can watch how the shoulder structures behave as you lift or rotate your arm.
It is cost-effective and highly accurate for detecting many rotator cuff tears. For many tendon-related issues, ultrasound provides nearly the same useful info as an MRI when it comes to guiding treatment decisions.
MRI
MRI provides detailed images of soft tissues, including tendons, ligaments, cartilage, and surrounding structures. It also gives a more comprehensive view of the joint.
MRI is typically used if surgery is being considered or if symptoms are not improving with conservative care. It can help clarify the situation when earlier imaging or treatment has not fully explained the problem.
Important principle:
Abnormal imaging ≠ automatic surgery.
And normal imaging ≠ “nothing is wrong.”
Clinical context is everything.
What You Can Do Right Now (Without Making It Worse)
If you don’t have red flags, most cases of shoulder pain when lifting your arm improve with smart adjustments.
Not total rest.
Not pushing through it.
Smart adjustment with rest and activity modification. But we always tell our fellow athletes, speak with your physical therapist, they will guide you on the best regimen while your shoulder heals.
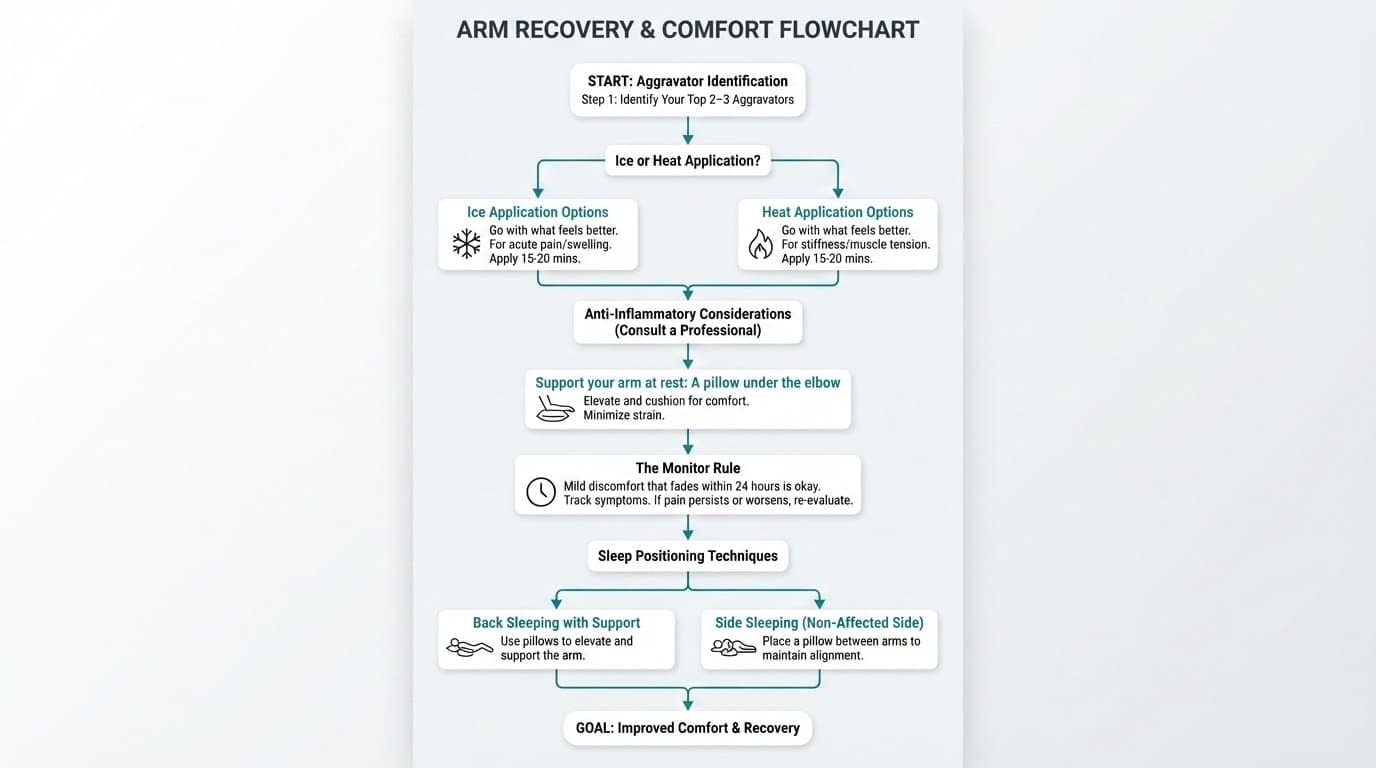
Step 1: Identify Your Top 2–3 Aggravators
Maybe it’s:
-
Heavy overhead pressing
-
Kipping pull-ups
-
Deep dips
-
Behind-the-neck movements
-
High-volume throwing
Temporarily reduce or modify them.
Quick Self-Care Moves That Actually Work
Here are some quick tactics you can use. But they should never replace medical attention if needed.
-
Ice or heat: Go with what feels better. No science says one is king over the other to relieve pain.
-
OTC anti-inflammatories: Only if they’re safe for you, of course.
-
Support your arm at rest: A pillow under the elbow while lying down can make a huge difference.
-
The “monitor rule”: Mild discomfort that fades within 24 hours is okay. Sharp spikes or lingering pain? Dial it back. However, this rule alone prevents 80% of flare cycles.
Sleep Smarter
Night pain often improves just by adjusting support.
-
Avoid lying directly on the painful shoulder
-
Support the arm with a pillow in front of your body
-
Avoid extreme stretched positions overnight
Keep It Moving (But Not Aggressively)
Total rest is tempting, but trust us: more than a few days of immobility usually just leads to stiffness. Instead, keep the joint happy with:
-
Gentle pendulum swings
-
Pain-free active range below shoulder height
-
Light isometric holds in comfortable positions
-
Short-range rowing movements (if tolerated)
Movement feeds circulation. Circulation supports tissue recovery.
Structured Recovery: What Actually Works
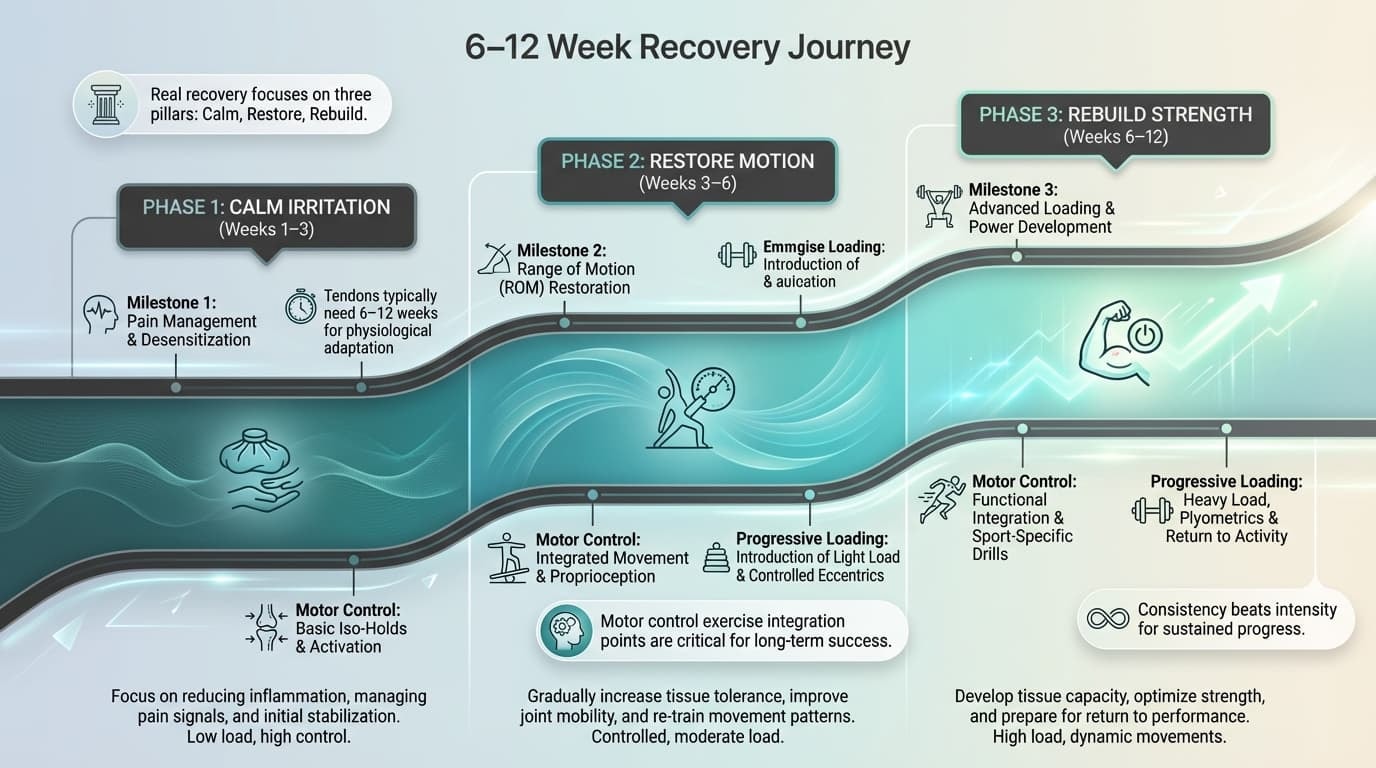
Real recovery focuses on three pillars:
-
Calm irritation
-
Restore motion
-
Rebuild strength
Physical therapy is often the most effective non-surgical approach.
A good plan includes:
-
Rotator cuff strengthening (especially external rotation work)
-
Scapular stabilization exercises
-
Gradual overhead reloading
-
Education on progression
Motor control exercise, teaching the shoulder blade and cuff to coordinate properly, consistently outperforms random stretching routines.
Tendons typically need 6–12 weeks of consistent, progressive loading to rebuild tolerance.
Consistency beats intensity.
Where the Anaconda Shoulder Brace Fits In
This is important.
A brace is not a replacement for rehab.
But during the rebuilding phase, when you’re returning to controlled training, added stability can reduce strain on irritated tissues.
The Anaconda Shoulder Brace uses 3D compression to:
-
Provide joint stability without bulk
-
Enhance proprioception (your body’s awareness of position)
-
Support circulation
-
Protect from impact using detachable gel padding
-
Stay secure during movement without restricting range
We designed it because we’ve lived through the mental side of injury.
Trying to train through instability is risky. Training with smart support while rebuilding strength is strategic.
Our promise isn’t to “fix” your shoulder.
Our promise is to help protect it while you do the real work, that is, the strengthening, the progression, the smart recovery.
Because at the end of the day, it’s about getting you back to doing what you love, confidently, safely, and for the long haul.
Frequently Asked Questions About Shoulder Pain When Lifting Your Arm
How does the Anaconda Shoulder Brace improve return-to-play timelines?
The Anaconda Shoulder Brace utilizes 3D compression to enhance proprioceptive feedback, which reduces the "apprehension" reflex during overhead movements. By stabilizing the glenohumeral joint without restricting functional range, it allows athletes to maintain training volume while overloaded tendons undergo the 6–12 week remodeling phase
At Anaconda, we know shoulder pain can feel frustrating and confusing. If you’re still unsure about what’s going on, you’re not alone. Here are clear answers to the questions we hear most often.
Can I distinguish between a cervical nerve referral and a shoulder tear at home?
Cervical referral often involves tingling or burning that radiates past the elbow, often triggered by neck rotation rather than arm movement. In our 2026 clinical observation, true shoulder pathology typically remains localized to the deltoid or AC joint and is primarily aggravated by manual resistance or reaching.
Do I Always Need an MRI for Shoulder Pain When I Lift My Arm?
No. Most people with gradual-onset shoulder pain when lifting the arm do not need an immediate MRI. Diagnosis is typically based on your symptoms and a physical examination. Guidelines recommend considering imaging only if pain hasn’t improved after roughly 6–12 weeks of appropriate care, if a large tear is suspected, or if surgery is being considered.
Ultrasound can often provide similar information to MRI for rotator cuff tears at a lower cost. Whatever the imaging modality, findings must be carefully matched to symptoms—many “abnormalities” on scans are incidental and don’t require treatment.
Why Is My Shoulder Pain Worse at Night, Especially When Lying Down?
Lying on the painful shoulder compresses irritated tendons or bursa, and relaxed muscles at night may allow the humeral head to shift slightly, increasing pressure in the subacromial space. Inflammation also tends to build when circulation slows during rest.
To reduce pain at night, use pillows to support your arm slightly away from your body, avoid prolonged lying on the painful side, and consider sleeping on your back or the unaffected side. As irritation settles with treatment and load changes, night pain typically improves. Persistent severe pain every night despite these adjustments should prompt professional review.
Can I Keep Working Out If My Shoulder Hurts When I Press or Lift Overhead?
Many people can safely continue training by removing or modifying the specific movements that reliably spike pain, usually heavy overhead presses, dips, or wide-grip bench. Maintain lower-body, core, and cardiovascular training to stay active.
Modifications that often help:
-
Reduce load and range of motion
-
Use neutral-grip dumbbells instead of barbells
-
Swap overhead pressing for pain-free horizontal pressing or pulling variations
-
Focus on scapular and rotator cuff strengthening exercises
Pushing through sharp pain or repeatedly “testing” the painful movement typically prolongs symptoms. A temporary deload paired with specific rehab work usually leads to better long-term performance.
How Long Does Rotator Cuff Tendinopathy or Shoulder Impingement Usually Take to Heal?
Milder cases often improve noticeably within 4–6 weeks with appropriate rest and targeted exercise. More persistent cases may take 3 months or longer to fully settle. Tendons are slow-healing tissues that respond best to gradual, progressive loading.
Progress is rarely perfectly linear. Occasional mild flare-ups are normal as activity increases, as long as pain returns to baseline within about 24 hours. Focus on function (better reach, improved strength, better sleep) rather than just pain scores. If there’s no clear progress over several weeks, seek professional input.
Will a Cortisone (Steroid) Injection Fix My Shoulder Pain Permanently?
Corticosteroid injections can provide short-term relief for some people, especially with subacromial bursitis or AC joint irritation. However, they don’t address underlying strength or movement issues, and research shows benefits typically last less than about 12 weeks on average.
Repeated injections carry potential risks, including tendon weakening and effects on blood sugar in people with diabetes. If an injection is used, it should be combined with a structured rehab program and activity modification, not viewed as a stand-alone cure.Do I Always Need an MRI for Shoulder Pain When I Lift My Arm?
No. Most people with gradual shoulder pain do not need an MRI right away. In many cases, a diagnosis can be made based on your symptoms and a thorough physical exam. Imaging is usually considered only if pain has not improved after about 6–12 weeks of appropriate care, if a significant tear is suspected, or if surgery is being discussed.
Ultrasound can often provide similar information to an MRI for rotator cuff tears, and it typically comes at a lower cost. No matter which imaging method is used, results must be interpreted carefully. Many “abnormal” findings on scans are common and not actually the cause of pain. Imaging should always match the clinical picture.
Why Is My Shoulder Pain Worse at Night, Especially When Lying Down?
Night pain is common with shoulder irritation. Lying directly on the painful shoulder can compress sensitive tendons or the bursa. When your muscles relax during sleep, there may also be slight changes in joint positioning that increase pressure in the shoulder. Inflammation can feel more noticeable at rest as well.
To reduce discomfort, try placing a pillow under your arm so it rests slightly away from your body. Avoid staying on the painful side for long periods. Sleeping on your back or on the opposite side is often more comfortable. As irritation improves with proper treatment and load management, night pain usually decreases. If severe pain continues despite adjustments, it’s worth getting professional guidance.
Can I Keep Working Out If My Shoulder Hurts When I Press or Lift Overhead?
In many cases, yes, with smart adjustments. The key is to remove or modify the specific movements that consistently trigger sharp pain. This often includes heavy overhead presses, dips, or wide-grip bench press variations. You can still train your lower body, core, and cardiovascular system to stay active.
Helpful modifications often include:
-
Reducing load and limiting range of motion
-
Using neutral-grip dumbbells instead of a barbell
-
Swapping overhead pressing for pain-free horizontal pressing or pulling movements
-
Prioritizing rotator cuff and shoulder blade strengthening
Pushing through sharp pain or repeatedly “testing” the painful movement usually delays recovery. A short period of reduced load combined with targeted rehab often leads to better long-term performance.
How Long Does Rotator Cuff Tendinopathy or Shoulder Impingement Take to Heal?
Milder cases often improve within 4–6 weeks when managed properly with rest and targeted exercise. More persistent cases may take three months or longer to fully settle. Tendons heal slowly and respond best to gradual, progressive loading.
Recovery is rarely perfectly smooth. Small flare-ups can happen as activity increases, as long as symptoms settle back to baseline within about 24 hours. Focus on overall function, better reach, improved strength, improved sleep, rather than pain alone. If there’s no clear progress after several weeks, professional input is recommended.
Will a Cortisone (Steroid) Injection Fix My Shoulder Pain Permanently?
Corticosteroid injections can provide short-term relief for some people, particularly in cases of bursitis or AC joint irritation. However, injections do not correct underlying strength or movement issues. Research shows the benefits are typically temporary, often lasting less than about 12 weeks.
Repeated injections can carry risks, including potential tendon weakening and effects on blood sugar in individuals with diabetes. If an injection is used, it should be part of a broader plan that includes structured rehabilitation and activity modification—not a stand-alone solution.Do I Always Need an MRI for Shoulder Pain When I Lift My Arm?
No. Most people with gradual shoulder pain don’t need an MRI right away. In many cases, we can figure out what’s going on based on your symptoms and a proper physical exam. Imaging is usually considered only if pain hasn’t improved after about 6–12 weeks of appropriate care, if a larger tear is suspected, or if surgery is being discussed.
An ultrasound can often provide similar information to an MRI when looking at rotator cuff tears, and it’s usually more affordable. No matter which scan is used, the results need to match your symptoms. Many “abnormal” findings show up on scans even in people without pain. Imaging should support the diagnosis, not drive it on its own.
Why Is My Shoulder Pain Worse at Night, Especially When Lying Down?
Night pain is common with shoulder irritation. Lying on the sore side can compress already sensitive tissues. When your muscles relax during sleep, the joint can also settle slightly, which may increase pressure in certain areas. Inflammation can simply feel more noticeable when everything else is quiet.
To make nights easier, try placing a pillow under your arm so it rests slightly away from your body. Avoid staying on the painful side for long periods. Sleeping on your back or the opposite side is often more comfortable. As your shoulder calms down and strength improves, night pain usually improves too. If it doesn’t, it’s worth getting checked.
Can I Keep Working Out If My Shoulder Hurts When I Press or Lift Overhead?
In many cases, yes, but you’ll need to adjust. Remove or modify the movements that clearly spike your pain. This is often heavy overhead presses, dips, or wide-grip bench press. You can still train your lower body, core, and cardio to stay active.
Helpful changes may include:
-
Reducing weight and limiting painful ranges
-
Using neutral-grip dumbbells instead of a barbell
-
Swapping overhead pressing for pain-free pressing or pulling variations
-
Focusing on rotator cuff and shoulder blade strength
Pushing through sharp pain or constantly “testing” the movement usually makes things worse. A short reset with smart rehab work often leads to better long-term results.
How Long Does Rotator Cuff Tendinopathy or Shoulder Impingement Take to Heal?
Milder cases often improve within 4–6 weeks with the right approach. More stubborn cases can take three months or longer. Tendons heal slowly and respond best to gradual, steady loading, not complete rest and not aggressive overload.
Recovery isn’t always perfectly smooth. Small flare-ups can happen as activity increases, as long as symptoms settle within about 24 hours. Look for progress in function, better reach, better strength, better sleep, not just pain levels. If you’re not seeing improvement after several weeks, get guidance.
Will a Cortisone (Steroid) Injection Fix My Shoulder Pain Permanently?
Cortisone injections can reduce pain in the short term, especially with bursitis or AC joint irritation. But they don’t fix the underlying strength or movement issues that often cause the problem. For many people, relief is temporary.
Repeated injections also carry risks, including possible tendon weakening and blood sugar changes in people with diabetes. If an injection is used, it should be part of a bigger plan that includes rehab and smart activity changes, not a quick fix on its own.













