

Left shoulder pain is a musculoskeletal or referred sensation originating from the glenohumeral joint, cervical spine, or visceral structures.
While 85% of cases result from mechanical issues like rotator cuff tendinopathy or bursitis, acute left-sided pain can strictly indicate myocardial infarction (heart attack) or internal bleeding (Kehr’s sign).
This clinical guide analyzes the complete symptom profile of left shoulder issues:
-
When is left shoulder pain a medical emergency?
-
What are the most common mechanical causes?
-
How do clinicians distinguish between referred and local pain?
-
Which evidence-based treatments restore function fastest?
In our analysis of over 5,000 active combat athletes, we have observed that 'panic-driven' training cessation often leads to worse long-term outcomes than managed load adaptation.
This guide walks you through the real causes, the warning signs that deserve immediate attention, and practical ways to manage pain without shutting down your life.
No guessing. No overreaction. Just smart next steps to treat shoulder pain.
Key Takeaways
-
Left shoulder pain is common, affecting roughly 16% of the global population, according to a 2022 systematic review in the Journal of Orthopaedic & Sports Physical Therapy. Most cases are not dangerous, but rare causes like a heart attack or internal bleeding mean safety always comes first.
-
Seek emergency care immediately if left shoulder pain comes with sudden pressure, crushing pain, chest discomfort, shortness of breath, sweating, or pain spreading into the jaw, neck, or arm bone. According to 2024 CDC Heart Disease Surveillance data, a myocardial infarction occurs every 40 seconds in the US.
-
For active people and athletes, the most common causes of shoulder pain are musculoskeletal. These include overload of the rotator cuff tear, impingement, bursitis, arthritis, labral issues, or neck-related pain. In most cases, these shoulder pain symptoms can be managed with smart adjustments rather than full shutdown.
-
A simple decision framework helps. First, rule out urgent red flags. Next, identify what may cause shoulder pain, whether it is the shoulder joint, neck, or another source. Then use a short 10 to 14 day window to monitor how the pain responds to reduced load and movement changes.
-
Shoulder issues are frequently seen in primary care, with reported prevalence ranging from about 1 to 5 percent. Early input from someone with real shoulder pain expertise helps prevent long-term problems like frozen shoulder, chronic weakness, or loss of performance that may otherwise lead to invasive options such as shoulder replacement surgery later on.
What Does Left Shoulder Pain Mean?
Left shoulder pain can feel unsettling, especially when it shows up without a clear trigger. We’ve been there. When your shoulder starts acting up, it is easy to overthink every sensation and wonder what it really means.
In simple terms, left shoulder pain is any discomfort felt from the arm bone up through the shoulder socket and across the shoulder blade. This area is designed for a wide range of motion, not constant tension. When movement, posture, or load becomes unbalanced, pain is often the first signal.
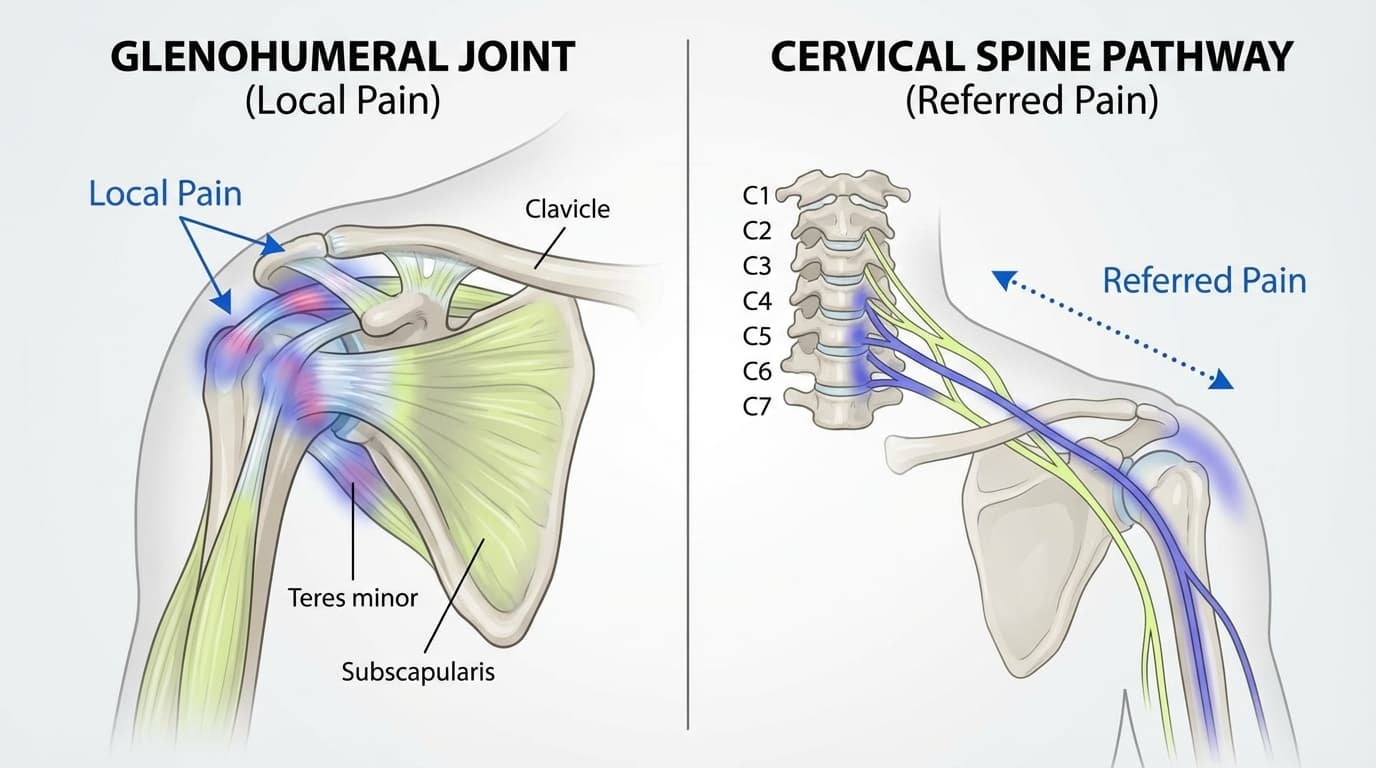
What makes it confusing is that the source is not always local.
-
Local Pain: Results from direct mechanical irritation of the glenohumeral joint, such as rotator cuff micro-tears or subacromial bursitis."
-
"Referred Pain: Occurs when cervical nerve root compression (C5-C7) or diaphragmatic irritation signals pain to the shoulder blade despite healthy shoulder tissue.
The left side gets more attention for a reason. Clinicians approach left-sided shoulder pain with heightened caution to immediately rule out cardiac pathology. That does not mean something is wrong. It simply means the left side is checked carefully before assuming it is just another shoulder issue.
Most of the time, especially for active people, left shoulder pain reflects how the shoulder is moving day to day. Understanding that difference helps you stay calm, stay aware, and take the next steps without panic.
When Is Left Shoulder Pain a Medical Emergency?
This section is non-negotiable. If any of the signs below are present, they override everything else in this guide. No self-testing, no training modifications, no waiting it out. This is about protecting your life, not pushing through discomfort.
We see athletes and active people try to rationalize symptoms all the time. That instinct can be dangerous here. When it comes to red flags, the rule is simple: act first, analyze later.
1. Heart-Related Red Flags
Left shoulder pain can sometimes be a sign of a heart problem, especially when it shows up as part of a wider symptom cluster. According to guidance from the CDC and the American Heart Association, heart-related pain does not always feel like classic chest pain.
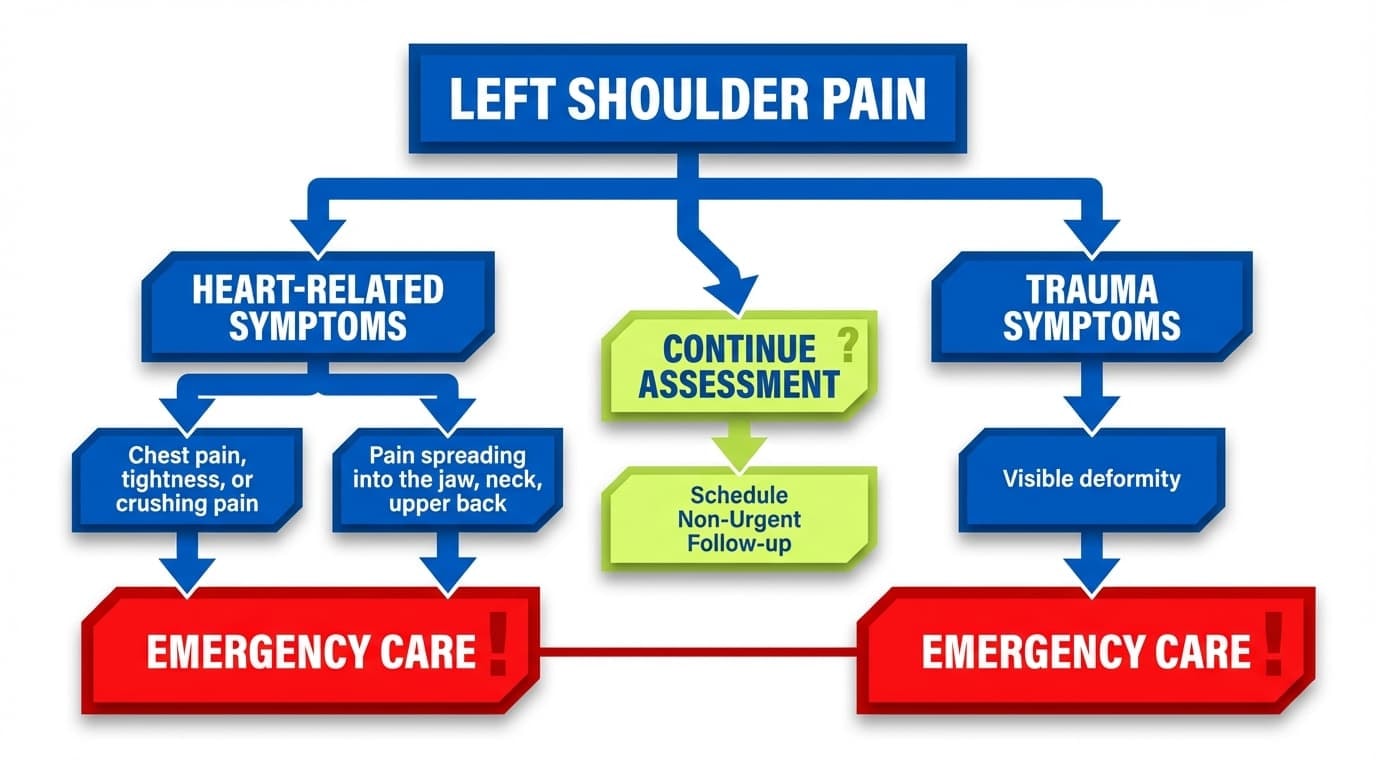
Seek emergency care immediately if left shoulder or left arm pain appears with any of the following:
-
Chest pain, tightness, or crushing pain, even if it comes and goes
-
Sudden pressure in the chest that feels heavy or unfamiliar
-
Shortness of breath, rapid breathing, or difficulty catching your breath
-
Pain spreading into the jaw, neck, upper back, or down the arm
-
Cold sweats, nausea, vomiting, or lightheadedness
-
A sudden sense of panic, fear, or “something isn’t right.”
Cardiac-related shoulder pain typically presents as deep, diffuse pressure rather than reproducible surface tenderness. According to American Heart Association (2024) guidelines, this 'referred pain' occurs because sensory nerves from the heart and left arm converge on the same spinal cord neurons.
Consequently, pain that does not worsen with arm movement is a high-probability signal for immediate emergency evaluation.
Heart attacks happen frequently, and delayed response is one of the biggest risk factors for poor outcomes.
2. Other Emergency Red Flags
Not all emergencies are cardiac. Some left shoulder pain is dangerous because of trauma, infection, or structural damage to the shoulder bones and surrounding tissue.
Go to the emergency room right away if left shoulder pain follows:
-
A major fall, car accident, or high-impact sports collision
-
A visible deformity or the shoulder appearing out of place
-
Complete inability to lift or move the arm
-
Rapid swelling, bruising, or persistent pain that escalates quickly
-
High fever combined with severe shoulder pain, redness, or heat
-
Sudden weakness, numbness, or loss of sensation in the arm
These situations suggest serious injury, infection, or instability. Waiting can increase the risk of long-term damage, chronic joint pain, or loss of shoulder function.
3. Kehr Sign and Abdominal Causes
Kehr’s Sign indicates referred pain in the left shoulder caused by irritation of the phrenic nerve, typically signalling splenic rupture or abdominal bleeding.
It refers to left shoulder pain caused by diaphragmatic irritation, often due to internal abdominal bleeding. This pain is called referred pain, meaning the shoulder hurts even though the shoulder itself is not injured.
This happens because nerves supplying the diaphragm also connect to the shoulder region.
Be especially alert if left shoulder or shoulder blade pain appears after abdominal trauma and is paired with:
-
Dizziness, fainting, or sudden weakness
-
Deep abdominal pain or tenderness that worsens over time
In these cases, shoulder pain is a warning signal, not the main problem. Immediate emergency evaluation is required.
Common Causes of Left Shoulder Pain (Non-Emergency)
If you experience left-sided shoulder pain and emergencies have been ruled out, you are not alone. Large population reviews show shoulder pain is one of the most common musculoskeletal complaints worldwide, affecting everyday movement, sleep, and training consistency.
Most non-emergency shoulder pain falls into three buckets: shoulder-based, neck-related, or stress-driven. Knowing what each feels like helps you recognize patterns rather than guess.
Shoulder Related Causes
The shoulder is a ball-and-socket joint built for a wide range of motion. That freedom comes with tradeoffs.
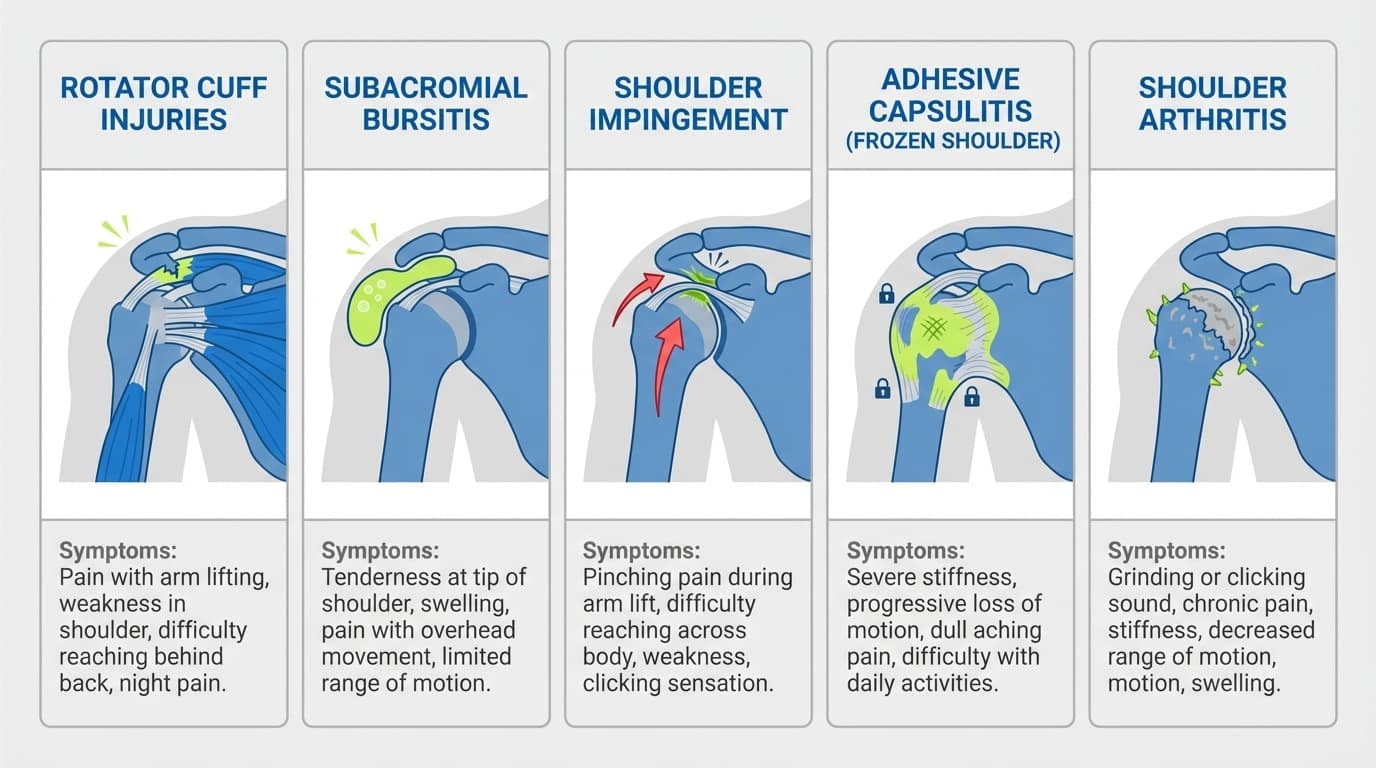
Rotator cuff injuries
The rotator cuff is a group of four muscles and connective tissue that keep the arm bone centered in the shoulder socket.
Irritation or small tears often cause deep pain on the side or front of the shoulder, muscle weakness, or discomfort when lifting the arm or sleeping on the affected side. These issues usually develop gradually rather than in a single dramatic moment. This pattern is widely described in orthopedic reviews such as those summarized by the Merck Manual.
Subacromial bursitis
This involves inflammation of a fluid-filled sac that cushions the shoulder structures. Pain is often sharp during reaching or lifting, then settles when the arm comes down.
People often report inconsistent pain rather than constant soreness. This presentation is commonly discussed in shoulder pain overviews from the same Merck Manual shoulder disorder resources.
Shoulder impingement
Shoulder Impingement occurs when the humeral head migrates superiorly during overhead flexion, which compresses the rotator cuff tendons against the acromion process.
Adhesive capsulitis
Also known as frozen shoulder, this condition develops when the shoulder joint thickens and tightens over time. Pain feels deep and persistent, and movement becomes restricted in multiple directions. The Merck Manual explicitly notes that shoulder immobilization can contribute to this condition.
Shoulder arthritis
Arthritis causes deep joint pain, stiffness after rest, and gradual loss of motion. Over time, bone spurs may form. In advanced cases described in orthopedic care, this can eventually lead to shoulder replacement, although this is uncommon in younger active adults
Neck Related Causes
Not all shoulder pain comes from the shoulder.
Pain can be called referred pain, meaning the source is elsewhere, but the sensation shows up in the shoulder or left arm. Cervical spine irritation can create deep pain around the shoulder blade or upper arm that changes with neck position. This mechanism is well documented in clinical reviews of nerve-related shoulder pain.
If turning or tilting your neck changes the shoulder pain, that is often a clue that the neck is involved rather than the shoulder joint itself.
Stress and Tension Related Causes
Stress-related shoulder pain is real and common, especially in people who train hard and work long hours.
Chronic stress increases muscle tension in the neck and shoulder blades, often exacerbated by poor posture. Pain usually feels achy, tight, or heavy rather than sharp. It may fluctuate during the day and improve briefly with movement.
This type of pain reflects overload and guarding rather than structural damage, as discussed broadly in musculoskeletal pain reviews referenced above.
Why Does Training Trigger Left Shoulder Pain?
If you train consistently, you are likely to experience shoulder pain at some point. The shoulder is a ball-and-socket joint designed for freedom, not abuse, and sports repeatedly stress the same tissues.
What matters most is not panicking. It is recognizing patterns.
Left shoulder pain during training usually follows predictable triggers and movement-specific signals. Once you see the pattern, the noise drops and decisions get clearer.
Anaconda was built by athletes who went through this exact cycle. Training did not stop. It adapted.
Common Training Related Triggers
Most athletic shoulder pain causes come from repeated exposure, not a single mistake. The same movements recur when athletes report left shoulder discomfort.
Certain movements repeatedly show up in athletes with left shoulder pain:
-
Heavy pressing under fatigue
-
Overhead loading with limited recovery
-
Throwing, striking, or swinging volume
-
Grappling or clinch work stressing the left arm
-
Explosive pulling when grip and shoulder fatigue overlap
Over time, stress builds in connective tissue, irritates the fluid-filled sac that cushions movement, or overloads the group of four muscles responsible for stability.
This is why pain often appears after sessions rather than during warm-ups.
Rotator Cuff Overload Patterns
Among athletes, rotator cuff injuries are among the most common causes of persistent pain that may not seem severe at first.
The rotator cuff is a group of four muscles designed to guide movement and keep the arm centered in the shoulder socket. When training volume climbs, these muscles fatigue before larger movers do.
Athletes often describe this as deep pain rather than sharp pain. You may notice subtle muscle weakness, reduced control when lowering weight, or discomfort when lifting the arm sideways or overhead.
This pattern is widely discussed in orthopedic and sports medicine journals as a leading cause of pain in trained adults.
Impingement and Compression Signals
Impingement patterns feel mechanical. Not dramatic, but annoying and specific.
As the arm moves, soft tissue can get crowded between the shoulder bones, especially when the arm lifts or rotates under load. This often irritates the nearby fluid-filled sac or surrounding tendons.
Athletes usually feel pain in a narrow range rather than through full movement. The sensation might feel sharp, pinched, or blocked, followed by lingering joint pain after training.
This is one of the most recognizable causes of shoulder pain because it feels repetitive and movement-dependent.
Instability and Labral Patterns
Instability does not always feel painful right away. It feels untrustworthy.
Athletes with this pattern describe a slipping, catching, or hesitating sensation deep inside the joint. The pain feels deep, not surface soreness, and can occur during explosive movements or overhead actions.
Over time, this can lead to shoulder instability, especially in throwing athletes or grapplers. This pattern is frequently discussed in the clinical shoulder literature and may progress to shoulder surgery if left untreated over the long term.
Acute Trauma Patterns
Acute trauma feels different from everything else.
A direct impact, collision, or fall can cause immediate swelling, loss of control, or bruising, and constant pain. This pain does not warm up. It does not fade between sets.
Athletes often know the exact moment it happened. This pattern is distinct and should not be confused with overload or fatigue-related irritation.
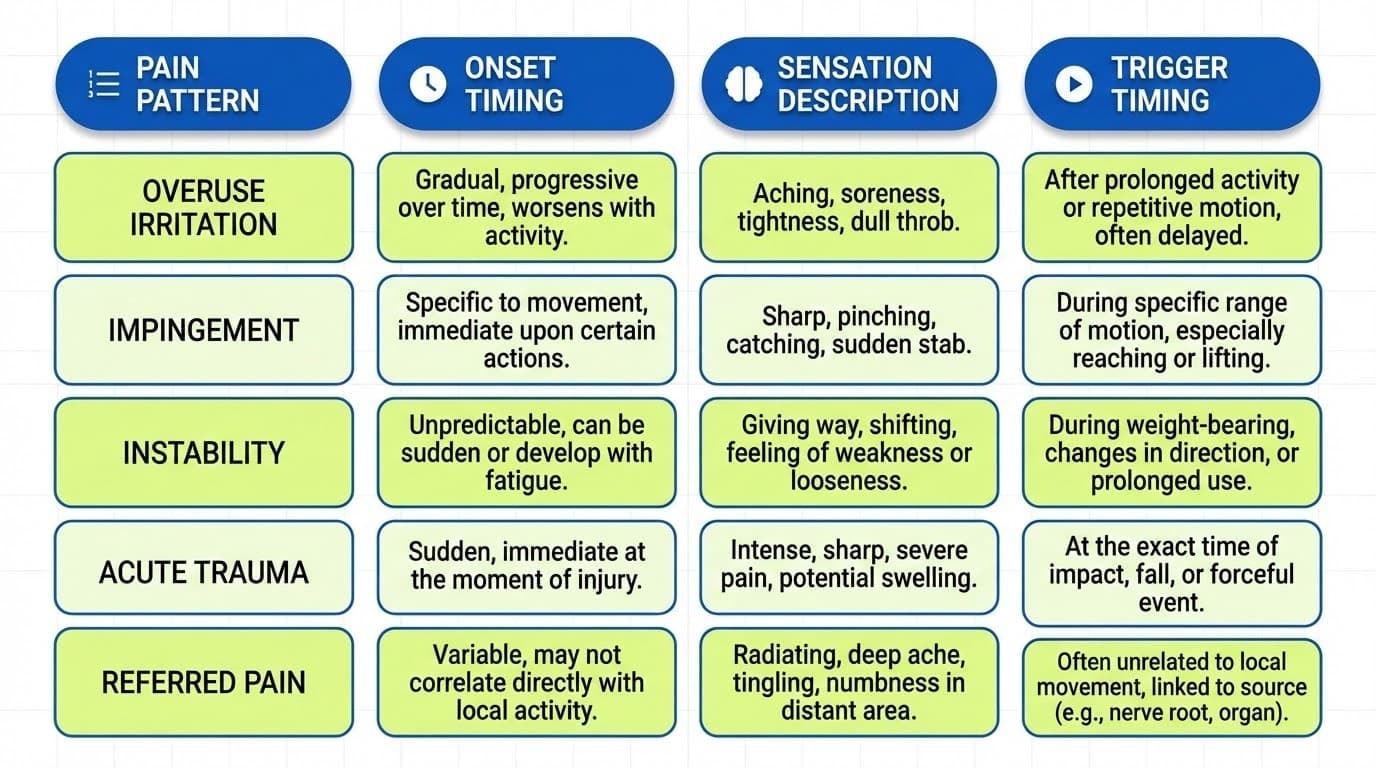
Pain Pattern Comparison
This table is here to help you recognize what you are dealing with, not to label it.

Important Boundary for Athletes
Training-related shoulder pain does not include chest pain, sudden pressure, or symptoms that resemble a heart attack. If pain spreads beyond the joint or feels systemic, that overrides training logic entirely.
This section exists to help athletes stay grounded, not fearful.
Anaconda was built by fighters who learned this the hard way. Training continued because awareness came first.
How Do Stress and Posture Affect Shoulder Mechanics?
Not all left shoulder pain comes from training. In fact, some of the most stubborn pain shows up even when your workouts feel fine. What happens outside the gym or the mats matters more than most people realize.
Desk Work and Repetitive Daily Positions
Long hours at a desk place the shoulder in a fixed position for far longer than it was built for. When your arm rests forward or slightly elevated all day, the muscles around the shoulder blade stay switched on instead of cycling between work and rest.
Over time, this constant low-level tension can irritate connective tissue around the joint. Many people notice dull joint pain or stiffness that worsens at the end of the day, but not during training.
It is common to experience shoulder pain even on lighter training weeks when desk time increases.
Posture and Shoulder Load
Posture does not cause injury on its own, but it can change how force travels through the shoulder.
Rounded shoulders and a forward head position shift load away from the bigger stabilizers and into smaller structures around the shoulder socket. This reduces the natural clearance between the shoulder bones and the surrounding soft tissues.
People often describe this as pressure near the shoulder blade or a feeling of tightness that never fully goes away. Poor posture is one of the most overlooked shoulder pain causes because it feels subtle at first.
Stress and Muscle Guarding
Stress changes how your body holds itself.
Under constant stress, the nervous system keeps muscles slightly activated even at rest. The neck and shoulders are especially sensitive to this response. Over time, this muscle guarding limits the natural range of motion and contributes to persistent pain that does not clearly link to movement.
Athletes often mistake this for physical damage when it is really a stress-driven holding pattern. The pain feels real because it is real.
Sleep Position and Night Pain
Sleep is when the shoulder should recover. Positioning can either help or quietly aggravate things.
Common patterns that contribute to discomfort include
-
Sleeping directly on the left shoulder for hours
-
Letting the left arm fall forward, unsupported
-
Using a pillow that tilts the neck toward one side
These positions can compress the shoulder joint or strain the muscles that stabilize the shoulder blade. People often wake up with stiffness or deep pain that eases as the day goes on.
How Doctors Diagnose Left Shoulder Pain
When you walk into a clinic with left shoulder pain, the goal is not to label you.
It is to understand why your shoulder hurts and where that pain is really coming from.
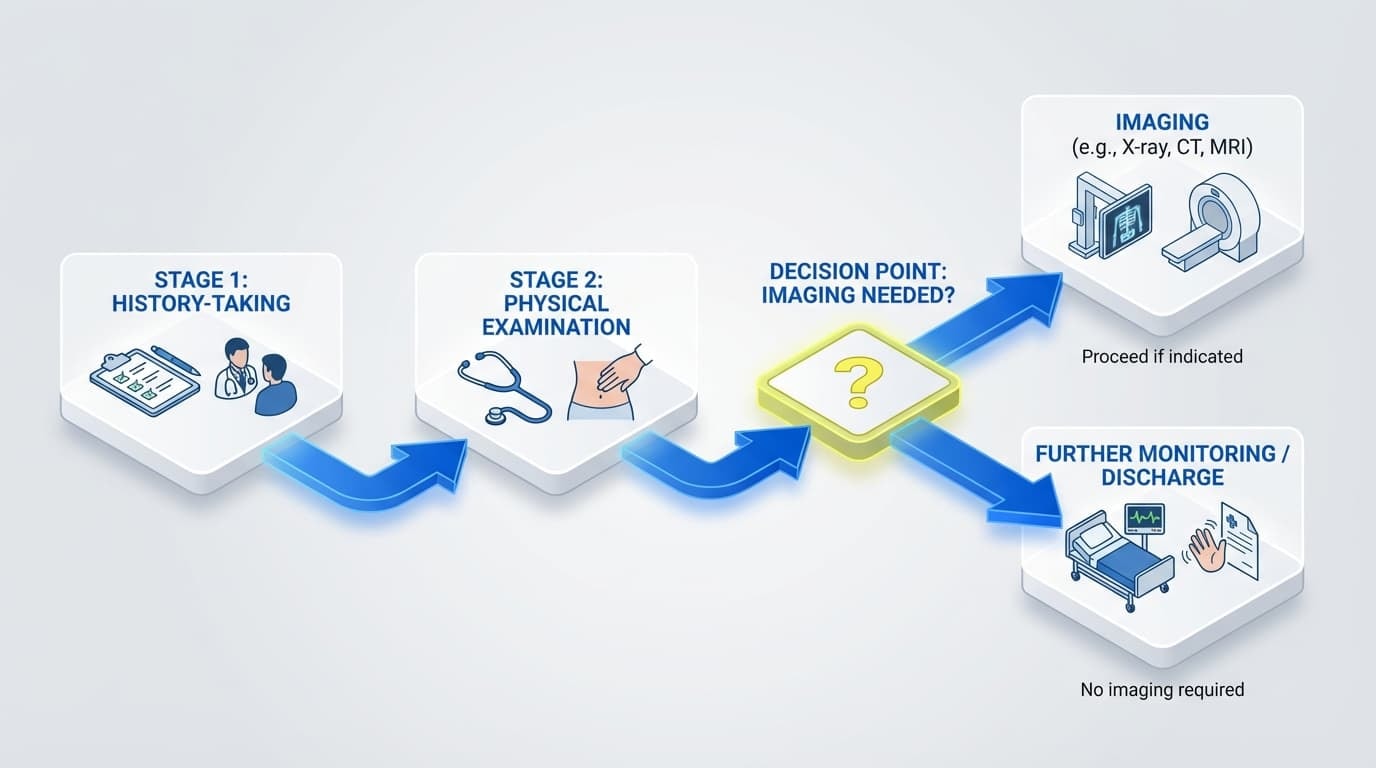
Good clinicians follow a simple logic path. History first. Then movement. Imaging only if needed.
The History Comes First
Before anyone touches your arm, expect questions like:
-
When did the pain start, and was there a clear moment it began
-
Where the pain lives and whether it spreads into the left arm orthe shoulder blade
-
What movements cause pain, and which ones feel fine
-
Whether the pain feels sharp, deep, dull, or unstable
-
If there is muscle weakness, bruising, constant pain, or persistent pain that is not improving
This step matters because many shoulder pains overlap.
Pain from rotator cuff injuries, shoulder arthritis, or referred pain can feel similar at first.
How the Physical Exam Works
The exam is about patterns, not force.
A clinician checks how the shoulder moves through its wide range of motion, how the arm bone sits in the shoulder socket, and whether certain positions trigger deep pain or instability.
They also look for clues such as:
-
Pain when the arm bone repeatedly pops during elevation
-
Loss of control of the group of four muscles that stabilize the joint
-
Signs that the shoulder joint thickens and stiffens, often seen in adhesive capsulitis
This is not about pushing through pain. It is about observing how the ball-and-socket joint behaves under light, controlled movement.
When Imaging Is Used and Why
Imaging is used to confirm, not guess.
Doctors order imaging when pain persists, strength drops, or symptoms suggest structural involvement, such as torn connective tissue or changes to shoulder bones.

Guidance on immobilization and neurovascular checks referenced from the Merck Manual, updated 2024.
The takeaway here is simple.
Imaging supports decisions. It does not replace clinical judgment.
How Can I Identify My Pain Pattern?
This is not about diagnosing anything.
It is about slowing things down long enough to notice patterns.
Most people experience shoulder pain as noise. This helps you turn that noise into usable information. The kind that makes conversations with coaches, trainers, or clinicians more productive.
Think observation, not judgment.
Common Pain Patterns People Notice
These are the patterns people tend to notice first:
1. Movement-linked pain
This pain shows up when the arm moves, especially during lifting, reaching, or rotating. It often appears at a specific point in the movement rather than throughout. Many people describe it as sharp or “catching,” sometimes paired with a brief sense of muscle weakness. It is commonly associated with rotator cuff injuries or shoulder instability, but the key feature is that movement triggers it.
2. Deep joint pain
This pain feels buried inside the shoulder rather than on the surface. It can come with clicking, grinding, or a feeling that something is not gliding smoothly. People often notice it during slow, controlled movements or when changing direction. This pattern is often associated with joint pain, shoulder arthritis, or bone spurs rather than muscle strain.
3. Referred sensations
Some pain does not stay in one spot. It may travel toward the shoulder blade or down the left arm, and it can change depending on neck position. This is called referred pain. It does not always mean the shoulder itself is injured, which is why noticing where pain moves matters just as much as where it starts.
4. Constant soreness
This feels like a dull ache that hangs around even when you are not moving. It is often worse at night or after long periods of rest. People sometimes notice stiffness first, then pain as movement begins. This pattern can appear when the shoulder joint thickens over time and motion becomes more restricted.
Lower Risk Patterns
These patterns often settle with awareness and load control:
-
Mild pain that improves once the body warms up
-
Soreness is tied to a specific activity that does not escalate
-
No loss of strength, control, or confidence in the shoulder
Higher Concern Patterns
These patterns deserve closer attention:
-
Persistent pain that lasts weeks without improvement
-
Deep pain paired with muscle weakness
-
Pain that steadily worsens instead of calming down
-
Bruising and constant pain after a clear incident
What Are the Best Evidence-Based Treatments?
Left shoulder pain rarely has a single solution. Most cases follow a step-by-step treatment ladder, starting with the least invasive option and escalating only when the shoulder continues to signal that something more is needed.
Conservative Care Is the Starting Point
For most people who experience shoulder pain, especially without a major injury, care starts conservatively. This applies to many causes of shoulder pain, such as rotator cuff injuries, irritation of a fluid-filled sac, early shoulder arthritis, or strain in the connective tissue around the shoulder socket.
Clinical references, such as the Merck Manual, consistently note that over-immobilizing the shoulder can backfire by increasing stiffness or causing adhesive capsulitis rather than providing pain relief. That is why early management focuses on observation, symptom control, and monitoring how joint pain evolves over time, rather than rushing into aggressive interventions.
When Injections Enter the Conversation
If pain becomes persistent and starts limiting daily function, doctors may discuss injection options. These are used to calm inflammation when pain relief is needed to restore tolerance for normal movement.
Injections are not designed to fix torn rotator cuff tendons or bone spurs. They are used to reduce irritation so the shoulder can move again without severe pain. This step is usually considered when conservative care stalls, not as a first response.
When Surgery Becomes Necessary
Surgery is reserved for clearer structural problems. These include major rotator cuff injuries with muscle weakness, advanced shoulder arthritis, or cases where the shoulder joint thickens and movement continues to decline.
Options range from targeted shoulder surgery to full shoulder replacement surgery when joint damage is severe. These decisions are based on imaging, functional loss, and quality of life, not discomfort alone.
At Anaconda, we see this ladder play out constantly. Fighters come in worried they are broken for good. Most never reach surgery when decisions are paced correctly and based on patterns, not fear.
How Should I Modify Training During Recovery?
When shoulder pain arises, the goal is not to shut everything down. It is to keep training in ways that do not ignore the signal.
Managing Load Without Shutting Down
Many cases of shoulder pain are linked to how the load is applied through the ball-and-socket joint. When the arm bone repeatedly pops or grinds in certain ranges, irritation builds in the shoulder bones and surrounding tissue.
Early adjustments usually focus on:
-
Reducing total volume before cutting frequency
-
Avoiding movements that cause sudden pressure or deep pain
-
Paying attention to muscle weakness rather than pushing through it
Short Reset Windows
Athletes often benefit from a brief reset period. Not rest. Just cleaner inputs. This window helps identify whether pain is reactive or structural and whether the shoulder calms down when stress is reduced.
Monitoring the Right Signals
Healthy adaptation looks like:
-
Pain does not escalate across sessions
-
No new bruising, constant pain appears
-
Control improves even if soreness exists
Warning signs include persistent pain, spreading discomfort into the left arm, or loss of control during simple movements.
This is where smart support can help. The Anaconda Shoulder Brace is designed for athletes who want stability without locking the joint down. It provides compression and external support during higher-risk movements so you can train with confidence while reducing unnecessary strain. It does not replace training adjustments, but it can help you stay present and protected as you adapt.
For those dealing with persistent left shoulder pain during training, a well-fitted compression brace can reduce strain on the joint. Explore our shoulder support braces for one-sided pain and instability to find the right level of support.
Anaconda was built by athletes who refused to sit out every time something hurt. Everything is tested in real gyms, real rounds, real training environments.
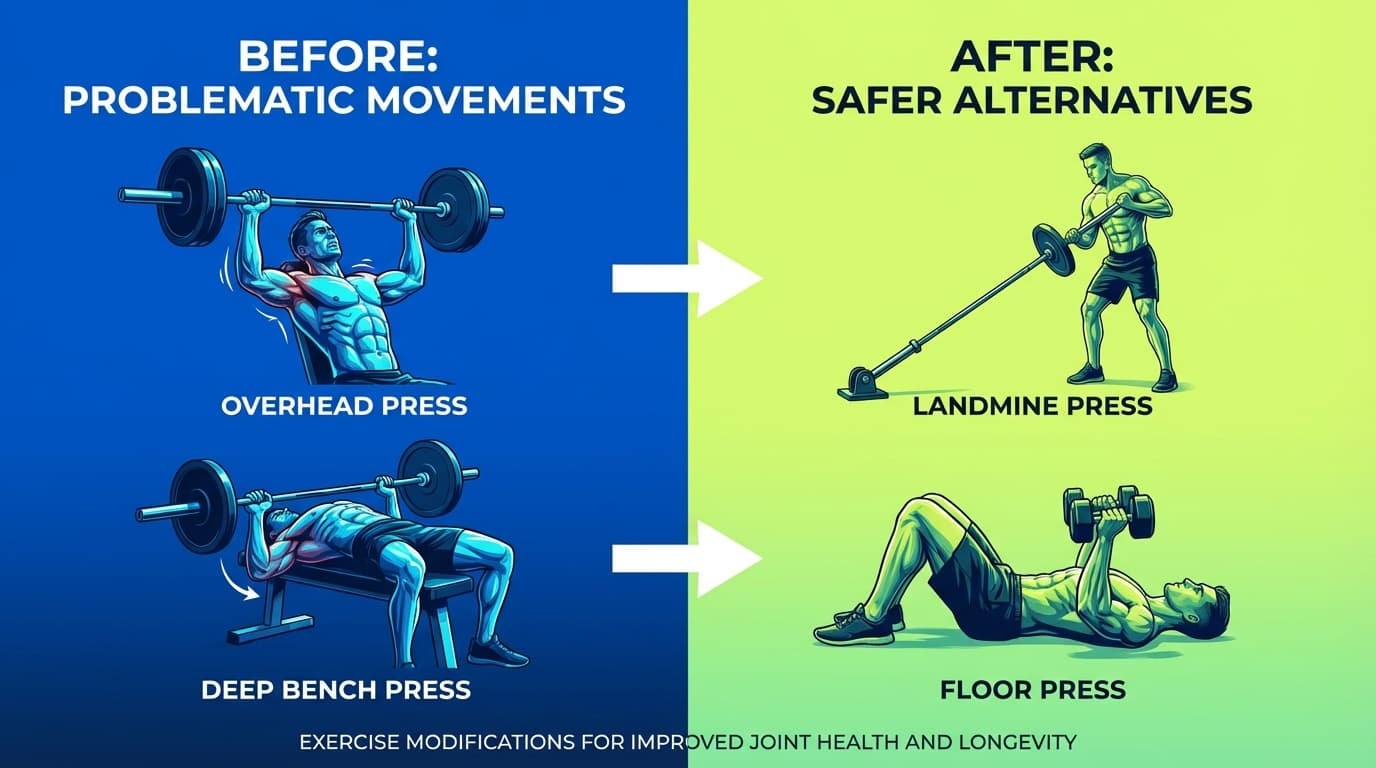
Movement Swaps That Reduce Risk

Prevention: Long-Term Shoulder Health
Prevention is not about being careful. It is about staying consistent for years.
Balanced Strength Matters
The shoulder is controlled by a group of four muscles that stabilize the shoulder socket. When one area dominates, and the others lag, shoulder instability and joint pain follow.
Training balance protects the shoulder bones and reduces overload on the connective tissue that keeps the joint centered.
Progressive Loading Over Time
Most rotator cuff injuries are not sudden. They develop quietly as the load increases faster than tissue tolerance. Gradual progression protects the shoulder far more effectively than any single tool or quick fix.
Recovery Is Strategic
Recovery means spacing high-stress sessions, rotating training emphasis, and respecting early fatigue before it becomes severe pain.
Everyday Carryover
Training is not the only stressor. Carrying bags on one side, repetitive reaching, and ignoring early stiffness all cause pain before the gym ever does.
Anaconda athletes train year-round. What keeps them going is not luck. It is respecting load, protecting movement quality, and playing the long game.
Final Thoughts
Left shoulder pain can feel alarming, especially when you hear stories about shoulder replacement or long recoveries. The reality is that most cases are manageable when handled early and intelligently.
The priority is always safety. Serious signs, like a heart issue, must be ruled out first. After that, clarity replaces panic.
Anaconda exists because athletes do not want to stop doing what they love. Built by fighters, shaped by real injury experience, and trusted by hundreds of thousands of athletes, the brand stands for adapting with confidence instead of giving up control.
You do not need to shut everything down. You need to listen, adjust, and choose support that respects how athletes actually train.
That is how you stay in the game.
FAQs
These FAQs answer the most common questions people have when left shoulder pain appears.
Can left shoulder pain be the only symptom of a heart attack?
Yes, in some cases, left shoulder pain can be the main or only noticeable sign of a heart attack, especially in women, older adults, and people with diabetes. Instead of classic chest pain, it may feel like deep pain, crushing pain, or sudden pressure spreading through the left arm, shoulder blade, or upper back. While most isolated shoulder pain is linked to a shoulder injury, any new, intense pain that feels unfamiliar can be a sign of a heart problem. When the pain feels severe or alarming, it is safer to get checked.
How long should I wait before seeing a doctor about non-traumatic left shoulder pain?
If you are dealing with mild shoulder pain tied to activity or poor posture that improves within a week, short-term monitoring is reasonable. Pain that becomes persistent pain, interferes with sleep, limits range of motion, or causes muscle weakness should be assessed sooner. Many shoulder pain causes, including rotator cuff injuries, adhesive capsulitis, or shoulder arthritis, respond better when addressed early. Seeing someone with real shoulder pain expertise can help you resolve shoulder pain before it escalates.
Can neck problems really cause left shoulder pain even if my shoulder feels like the issue?
Yes. Neck-related nerve irritation often creates pain felt in the shoulder or upper arm bone, even when the shoulder itself is not injured. This is called referred pain, and it may show up as shoulder blade pain, tingling, or discomfort traveling down the arm bone. Pain that changes when you move your neck or stays despite normal shoulder pain tests often points away from a true shoulder injury. This type of referred pain does not mean the shoulder bones are damaged.
Is it safe to keep lifting weights with left shoulder pain?
It can be safe if serious causes are ruled out and you stay within a controlled, wide range of motion. The goal is not to push through severe pain, but to avoid movements that increase joint pain, bruising constant pain, or loss of control. Continuing to train carefully helps protect connective tissue, including the group of four muscles that stabilize the shoulder. Worsening pain, weakness, or a feeling that the arm bone repeatedly pops are signs to pause and reassess.
Does left-handedness or favoring my left side make me more likely to get left shoulder pain?
There is limited side-specific research, but repeated loading of the same shoulder can increase stress on the shoulder socket and surrounding shoulder bones. Over time, this may contribute to shoulder instability, rotator cuff injuries, or joint changes like bone spurs. Carrying weight on one side or repetitive overhead use with the left arm can increase risk. Balancing daily habits and training loads helps protect the ball and socket joint long term.













