

Most common shoulder injuries follow a predictable pattern: they are either gradual overuse issues (like tendinopathy) or sudden traumatic events (like dislocations). Understanding this distinction is the fastest way to identify whether you need immediate medical attention or a structured load-management plan.
One week, it is a mild pinch when you press overhead. The next, it is waking you up at night. You start searching, and suddenly you are buried in terms like rotator cuff tear, impingement, frozen shoulder, and labral injury. It all sounds serious, and it is hard to tell what actually applies to you.
The truth is, most shoulder injuries follow patterns. They feel confusing at first, but they are rarely random.
At Anaconda Fightwear, we work with over 300,000 athletes managing shoulder stress from training, contact sports, and overhead work. Most shoulder injuries follow predictable patterns. Once you recognize the pattern, the path forward becomes much clearer.
This guide will help you sort what hurts, why it likely happened, and what to do next without overreacting or ignoring something important.
Key Takeaways
-
The most common shoulder injuries are usually overuse-related, not catastrophic tears. Understanding whether your pain started gradually or after trauma helps narrow the cause quickly and avoid unnecessary panic.
-
Changes in the glenoid labrum or signs of a rotator cuff injury on a scan do not automatically explain your pain. Diagnostic accuracy improves when imaging is combined with a physical exam, a positive test, and movement assessment, not used in isolation.
In cases like traumatic anterior shoulder instability, the ligaments holding the joint and the glenoid labrum are often involved. That is why some instability cases feel mechanical rather than just painful. -
Physical therapy remains one of the most effective first-line treatment approaches for reducing pain, restoring strength, and rebuilding confidence. For many athletes, structured rehab prevents the need for surgery altogether.
While advanced procedures are supported in some contexts by organizations like the American Shoulder and Elbow Surgeons, there is limited evidence that early surgery is necessary for most non-traumatic cases. Early load management, guided rehab, and intelligent training decisions usually come first.
Why Are Shoulder Injuries So Common in Athletes?
Anatomy explains why common shoulder injuries occur so frequently in athletes and active adults.
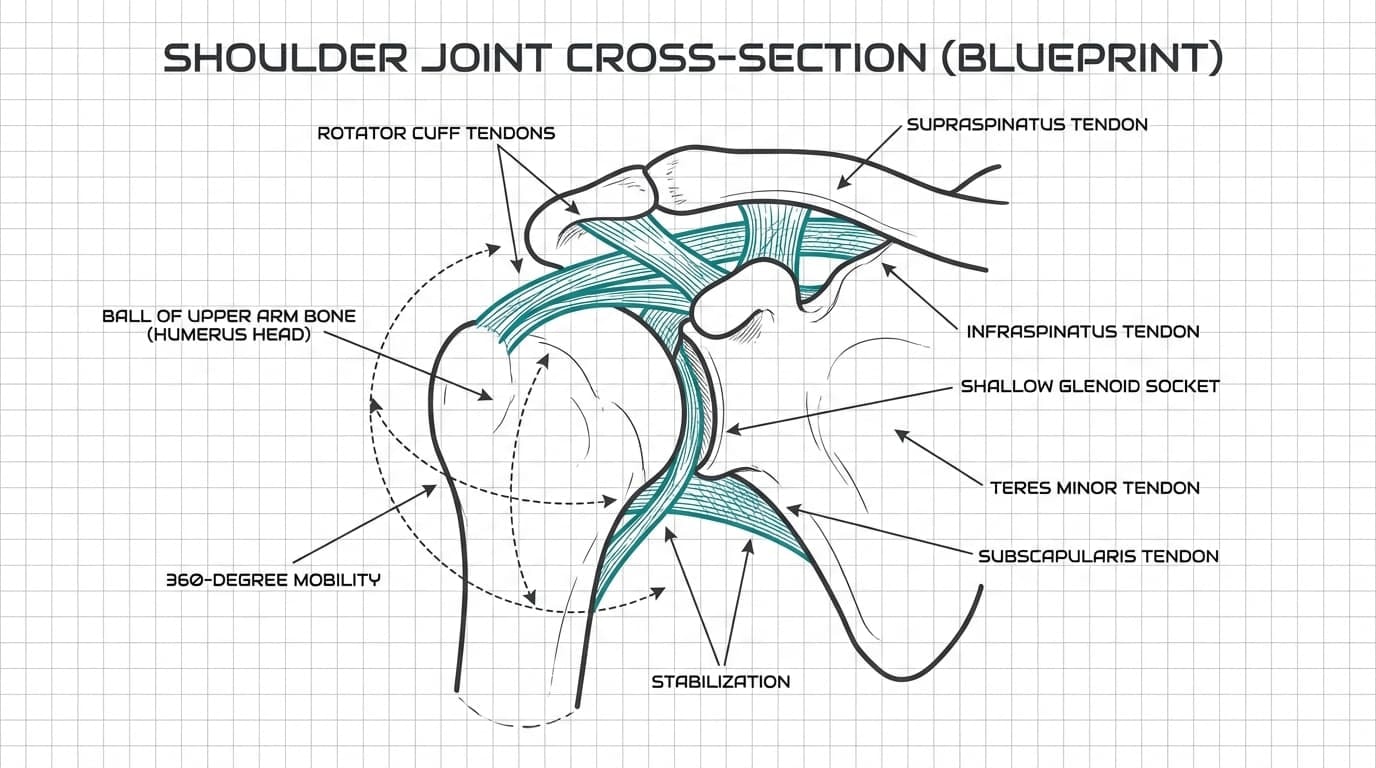
The shoulder (glenohumeral) joint is structurally defined by a shallow socket (glenoid) that sacrifices stability for 360-degree mobility. Because the bone contact is minimal, the joint relies almost entirely on soft tissues—specifically the rotator cuff tendons—to maintain joint centration during overhead load.
Unlike the hip, the ball of the upper arm bone sits in a relatively shallow socket on the shoulder blade. That design allows you to throw, press, swim, grapple, and rotate freely. But it also means the joint depends heavily on soft tissues for control.
Those soft tissues include the rotator cuff, which wraps around the upper arm bone and keeps it centered in the shoulder joint during movement. The rotator cuff works every time you lift your upper arm, reach overhead, or stabilize weight. Over time, repeated load can irritate these tendons and lead to some of the most common shoulder injuries seen in training environments.
That is why shoulder injuries tend to fall into predictable categories:
-
Overuse-related rotator cuff irritation
-
Partial or full rotator cuff tear
-
Shoulder dislocation or instability
-
Frozen shoulder with progressive stiffness
-
Degenerative joint changes
Many shoulder injuries are not caused by one dramatic moment. They build gradually from repeated stress on the rotator cuff and surrounding structures. Others, like a shoulder dislocation, usually follow trauma such as a fall or collision.
Understanding this mechanical reality helps reduce panic. Not all shoulder pain means a severe rotator cuff tear. Not all stiffness means frozen shoulder. And not every click signals structural damage.
When you understand how the shoulder joint works, you can see why these common shoulder injuries develop and why most respond well to structured recovery rather than immediate surgery.
How to Quickly Sort Shoulder Pain: Overuse vs Trauma
When shoulder pain shows up, most people immediately jump to worst-case scenarios. Torn rotator cuff. Labrum damage. Something serious.
Before going there, slow down.
The most important question is simple: How did it start?
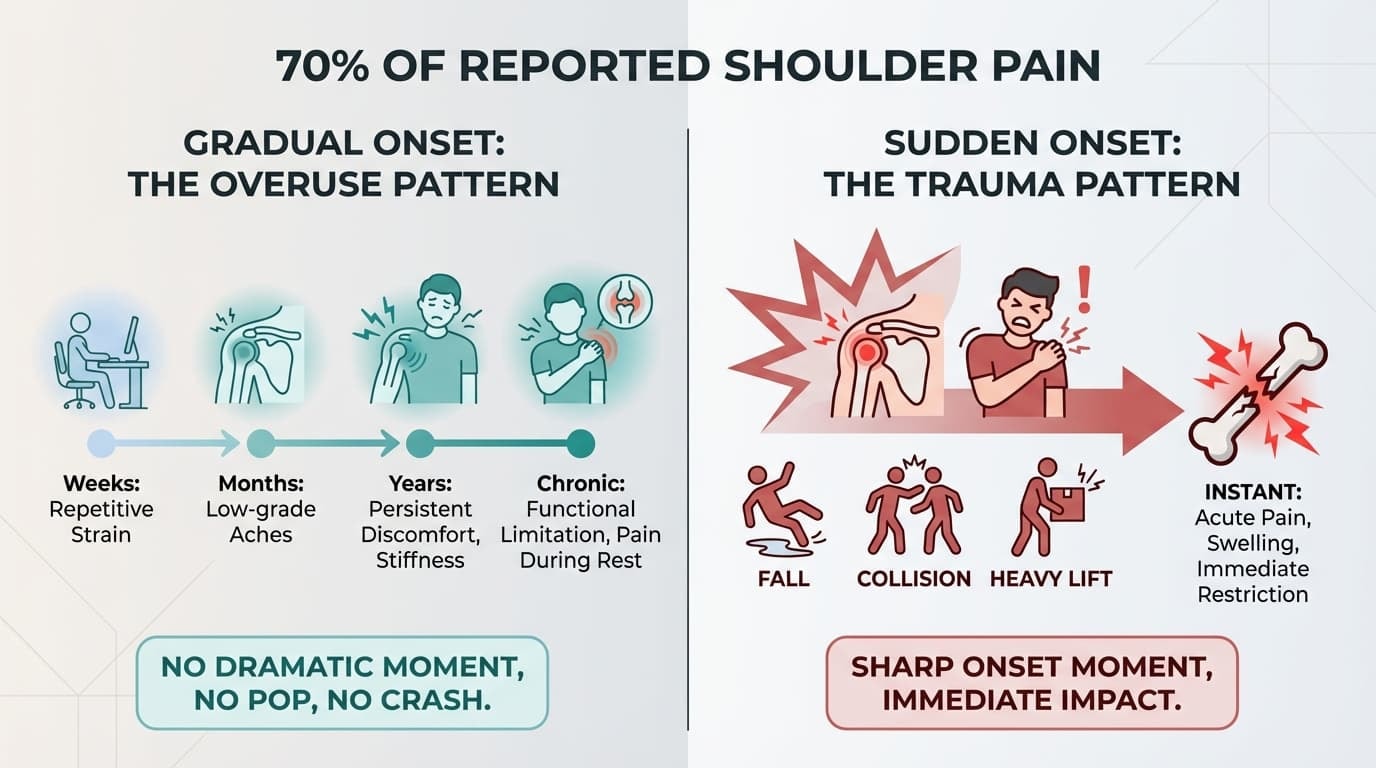
At Anaconda Fightwear, we have collected feedback from over 300,000 athletes since 2020. Our internal data suggests that 70% of reported shoulder pain stems from gradual volume overload rather than acute trauma. In most cases, the origin story tells you more than any online search ever could.
1. Gradual Onset: The Overuse Pattern
If your shoulder pain builds up slowly, this is usually an overuse pattern.
There was no dramatic moment. No pop. No crash. Just a shoulder that started feeling tight, irritated, or weak over time.
This commonly happens when:
-
Training volume increases too fast
-
Overhead lifts are added without proper progression
-
Throwing or swimming reps increase
-
Desk posture and heavy training combine
-
Recovery and mobility work are neglected
The shoulder joint depends heavily on the rotator cuff and shoulder blade muscles for control. When those muscles fatigue or lose coordination, stress on the tendons and the upper arm bone increases.
Common signs of overuse shoulder injuries:
-
Dull ache on the front or side of the shoulder
-
Pain when lifting the upper arm overhead
-
A “painful arc” between shoulder height and ear level
-
Night discomfort when lying on the affected side
-
Strength that feels limited because of pain, not true muscle failure
Overuse of shoulder injuries usually allow movement, but certain ranges feel irritated. You can often still train, just not pain-free.
The key with this pattern is intelligent modification, not full shutdown.
2. Sudden Onset: The Trauma Pattern
If you can point to the exact second it happened, that changes the picture.
Traumatic shoulder injuries typically involve:
-
A fall onto the shoulder or outstretched arm
-
A collision in contact sports
-
A heavy lift that suddenly overloaded the joint
-
Feeling the shoulder shift, pop, or move out of place
This pattern may involve a shoulder dislocation, an acute rotator cuff tear, a labral injury, or a fracture.
-
Acute Pain Onset: Immediate, sharp distress localized to the joint."
-
"Structural Deformity: Visible changes in shoulder contour or swelling."
-
"Functional Loss: Immediate inability to lift the arm or significant weakness."
-
"Instability Sensation: A feeling that the joint has shifted or 'popped' out of the glenoid.
Unlike gradual shoulder pain, trauma often causes sudden loss of function. The shoulder joint may not feel trustworthy.
That difference matters.
Why This First Question Matters
Gradual overuse shoulder injuries often improve with load management, mobility work, and structured strengthening.
Sudden trauma patterns deserve faster evaluation, especially if strength is significantly reduced or the shoulder feels unstable.
Understanding how your shoulder injuries started helps you choose the right first step.
That clarity alone reduces anxiety and prevents unnecessary panic.
Pattern first. Then plan.
Overuse Shoulder Injuries: Impingement, Tendinitis, and Bursitis
Most common shoulder injuries are not dramatic tears. They build slowly.
You do not remember one specific moment. Instead, the shoulder pain creeps in. A pinch when pressing overhead. An ache after training. Tightness that does not fully go away.
This pattern usually points to overuse shoulder injuries such as impingement, rotator cuff tendinitis, or bursitis.
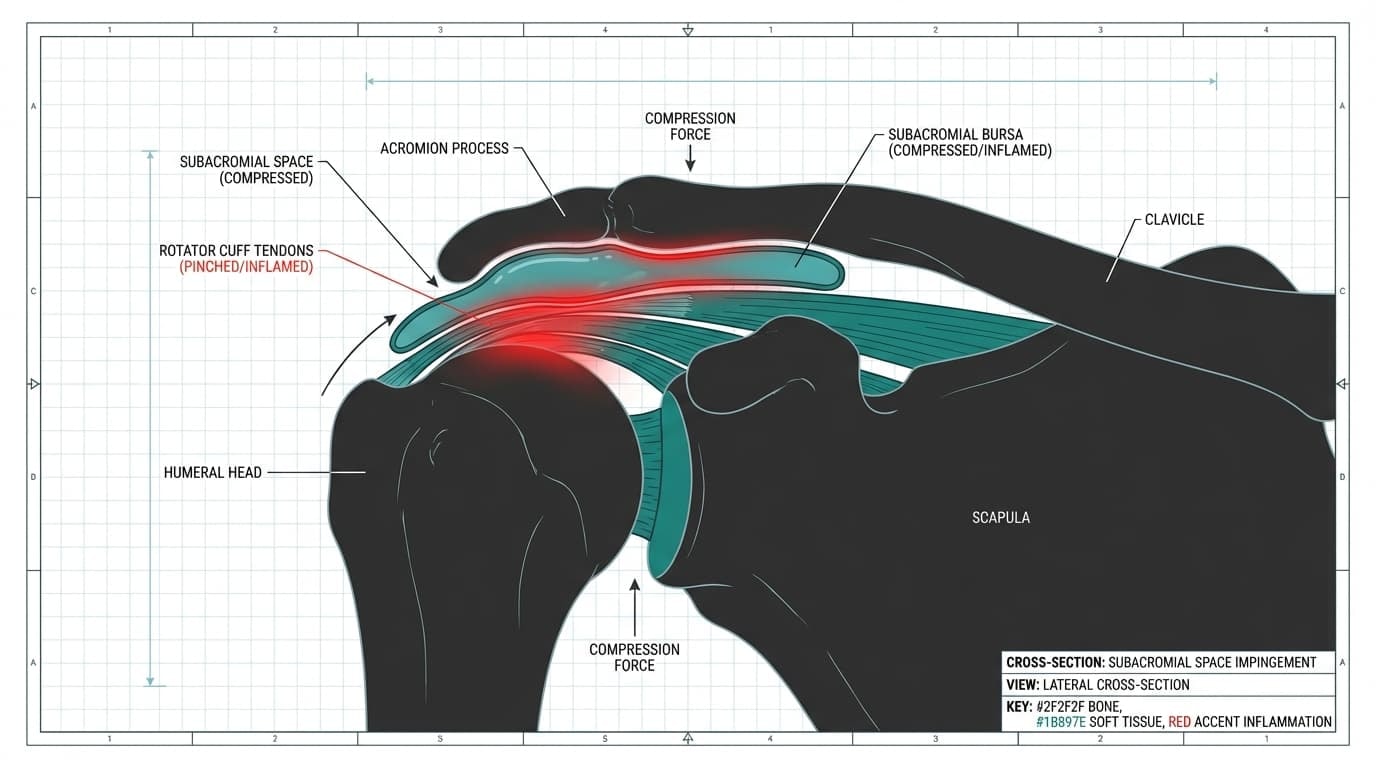
What Is Actually Happening
In Subacromial Impingement, the rotator cuff tendons and subacromial bursa become compressed within the narrow subacromial space, located between the humeral head and the acromion process. Every time you lift your upper arm, those tissues move through that space.
Rapid spikes in training volume or poor scapular mechanics inflame the tendons, causing the humeral head to migrate upward and impinge on sensitive soft tissue.
The rotator cuff works harder to stabilize the shoulder joint, inflammation builds, and the upper arm bone can press upward into sensitive tissue.
Over time, that irritation turns into persistent shoulder pain.
Common Symptoms
Overuse shoulder injuries usually show up as:
-
Dull ache at the front or side of the shoulder
-
Pain in lifting the upper arm overhead
-
Discomfort reaching behind your back
-
Night pain when lying on the affected side
-
Weakness that feels pain-limited rather than true muscle failure
These are extremely common shoulder injuries in weightlifters, swimmers, throwers, and anyone doing repetitive overhead work.
First-Line Conservative Care
The goal early on is not to shut everything down. It is to reduce irritation while keeping the shoulder joint moving.
Start with:
-
Temporarily reducing heavy overhead lifts
-
Avoiding movements that trigger sharp pain
-
Maintaining a pain-free range of motion
-
Beginning controlled rotator cuff and shoulder blade strengthening
Structured physical therapy can help restore balance between the rotator cuff, shoulder blade stabilizers, and surrounding muscles. Most overuse shoulder injuries improve when the load is managed intelligently.
During early load modification, some athletes use structured compression support to reduce joint strain while continuing light movement. A brace like the Anaconda Shoulder Brace provides 3D compression and stabilization without limiting the range of motion. It is not a replacement for rehab, but it can reduce irritation during the transition phase.
Overuse shoulder injuries are frustrating, but they are also highly responsive to smart adjustments. The key is addressing the root cause early, before minor irritation turns into something more serious.
Rotator Cuff Strains and Tears
Among common shoulder injuries, rotator cuff strains and tears create the most anxiety. The rotator cuff is a group of four muscles that stabilize the shoulder inside the shallow glenoid cavity while you lift and rotate your arm. When these tissues are irritated or torn, pain often appears with lifting, reaching, or lowering the arm under control.
The Imaging Myth: Not Every Tear Hurts
Before you panic about a scan result, here is something important.
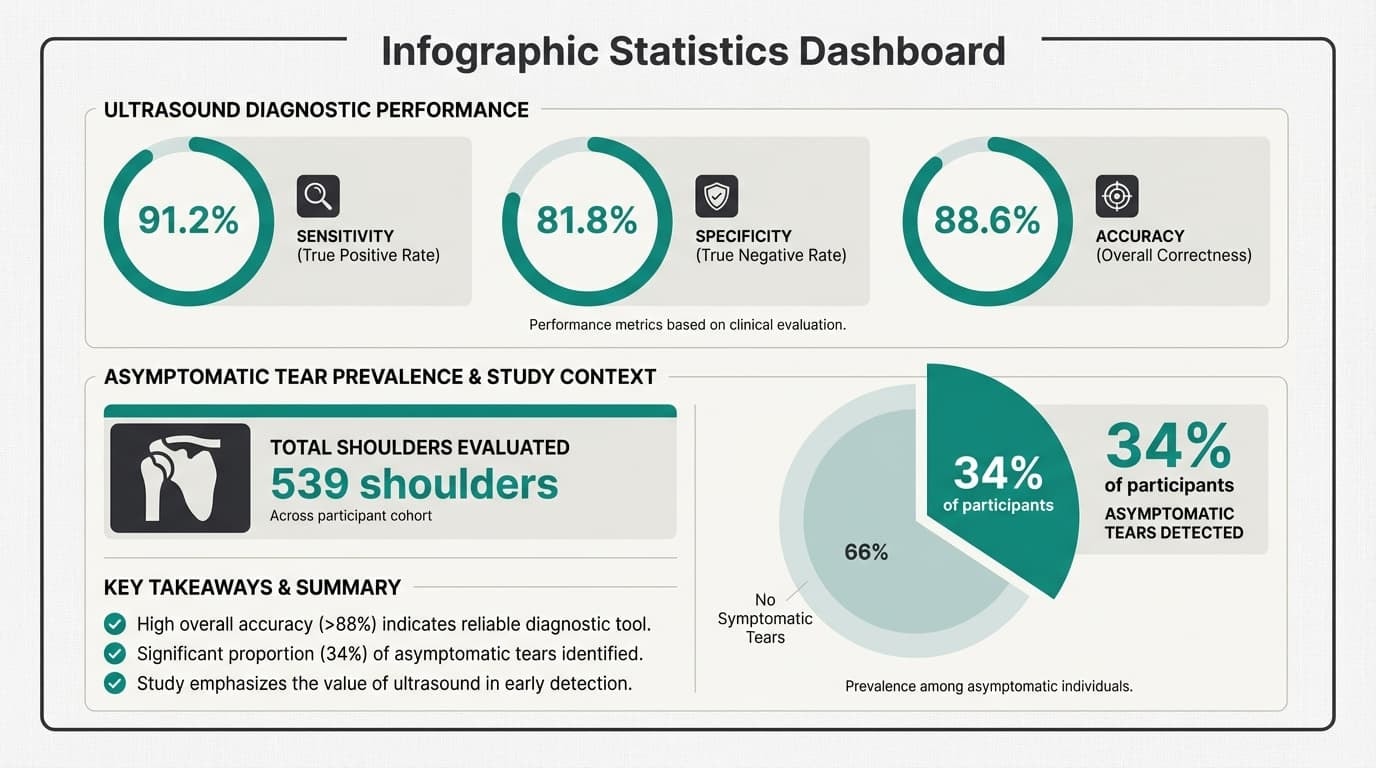
A 2025 population-based ultrasound study published in [Insert Journal Name, e.g., Journal of Shoulder and Elbow Surgery] analyzed 539 shoulders and found that 34% of participants had asymptomatic rotator cuff tears.
In other words, imaging findings do not automatically equal symptoms.
This is where context matters. A scan might show a structural change, but your actual pain pattern, strength, and function determine whether that finding is clinically meaningful. Imaging supports decision-making. It does not replace clinical reasoning.
Acute Injury vs Degenerative Wear
According to the AAOS OrthoInfo consensus, there are two main causes of rotator cuff tears: injury (acute) and wear (degeneration).
An acute injury usually follows a clear event. A heavy lift. A fall. A sudden pull. Pain is sharp, strength drops, and raising the arm becomes difficult.
Degenerative tears develop gradually. Over time, repetitive loading weakens tendon tissue. Then one movement becomes the tipping point.
Both patterns are common shoulder problems in athletes and active adults. The key difference is how they start and how aggressively they affect arm strength.
MRI vs Ultrasound: What Actually Works?
When imaging is appropriate, both MRI and ultrasound are commonly used in sports med and orthopedic settings.
A 2024 diagnostic comparison study of 53 patients found:
-
Ultrasound sensitivity: 91.2%
-
Specificity: 81.8%
-
Overall diagnostic accuracy: 88.6%
That means ultrasound performs very well in identifying rotator cuff tears when done properly. MRI provides more detailed structural information, but ultrasound remains a strong option with excellent diagnostic accuracy.
The takeaway is simple. Imaging can be useful, but it must be interpreted alongside your symptoms, physical exam, and injury history. Many systematic review analyses and cohort studies in sports medicine emphasize this same principle. There is limited evidence that imaging alone predicts pain severity or recovery.
What Treatment Typically Includes
For many partial tears and strains, treatment includes:
-
Load modification
-
Progressive strengthening
-
Gradual return to overhead activity
-
Guided physical therapy
More significant tears may require surgical consultation, particularly if arm weakness persists after conservative medical care.
Rotator cuff injuries can sound intimidating. But not every tear is catastrophic. Understanding the difference between structural change and meaningful dysfunction is what keeps you from overreacting and helps you choose the right next step.
Alongside physiotherapy and rest, wearing the right compression brace can significantly reduce re-injury risk — our upper body supports for common shoulder injuries are designed to stabilize the joint during training and daily activity.
Shoulder Instability and Dislocations
Shoulder instability happens when the ball of the upper arm bone moves excessively within the shoulder joint, or fully slips out of the glenoid cavity. When it completely comes out, that is a shoulder dislocation. These injuries are most common in athletes involved in contact sports or high-speed activities.
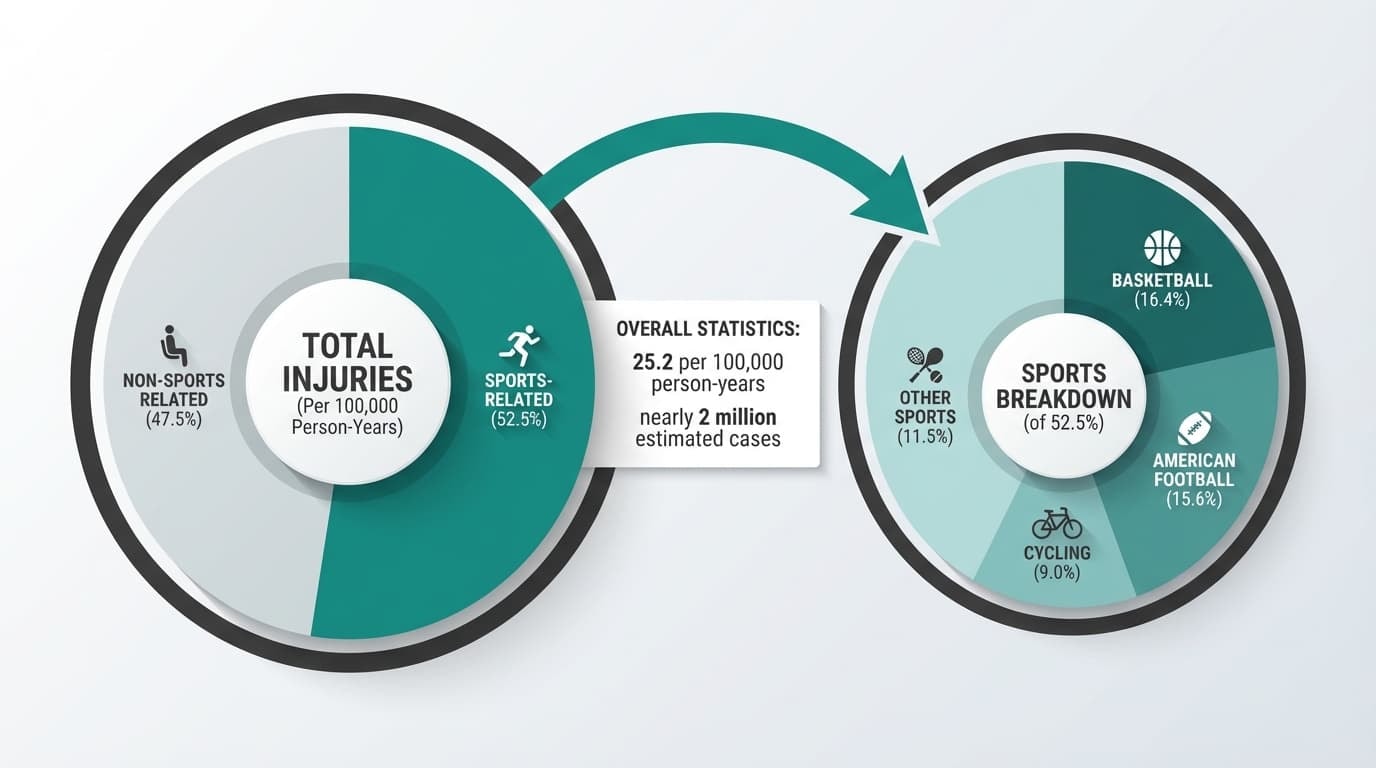
A 2024 national emergency department analysis reported a shoulder dislocation incidence of 25.2 per 100,000 person-years, representing nearly 2 million estimated cases nationally. Importantly, 52.5% were sports-related, with:
-
Basketball accounting for 16.4%
-
American football 15.6%
-
Cycling 9%
That data reinforces what sports med clinicians already see daily. Instability is strongly linked to athletic activity.
How Shoulder Dislocation Usually Happens
Most shoulder dislocations occur when the arm is forced backward and outward, placing stress on the ligaments holding the joint in place. Common mechanisms include:
-
Falling on an outstretched arm
-
A collision during football, rugby, or basketball
-
High-speed cycling or skiing crashes
-
Blocking or overhead contact in court sports
Anterior instability is the most common pattern, meaning the upper arm bone shifts forward out of the socket.
What It Feels Like
Acute shoulder dislocation often presents with:
-
Sudden severe pain
-
A visible change in the shoulder contour
-
Inability to move the arm
-
A “popped out” sensation
-
Possible numbness or tingling down the arm
Recurrent instability feels different. The shoulder may not fully dislocate, but can feel like it is slipping or “giving way” during overhead movements. Athletes often describe apprehension when the arm is placed in a throwing position.
Why Recurrence Matters
Once the shoulder dislocates, structures such as the glenoid labrum or the capsule can be injured. This increases the risk of repeat episodes, especially in younger athletes. Early structured rehabilitation is critical to restore strength and dynamic stability.
If you suspect a true dislocation, seek immediate medical care. Reduction must be performed safely to prevent nerve or vascular injury.
For athletes, recognizing instability early helps prevent repeated injury and long-term joint damage.
Frozen Shoulder (Adhesive Capsulitis)
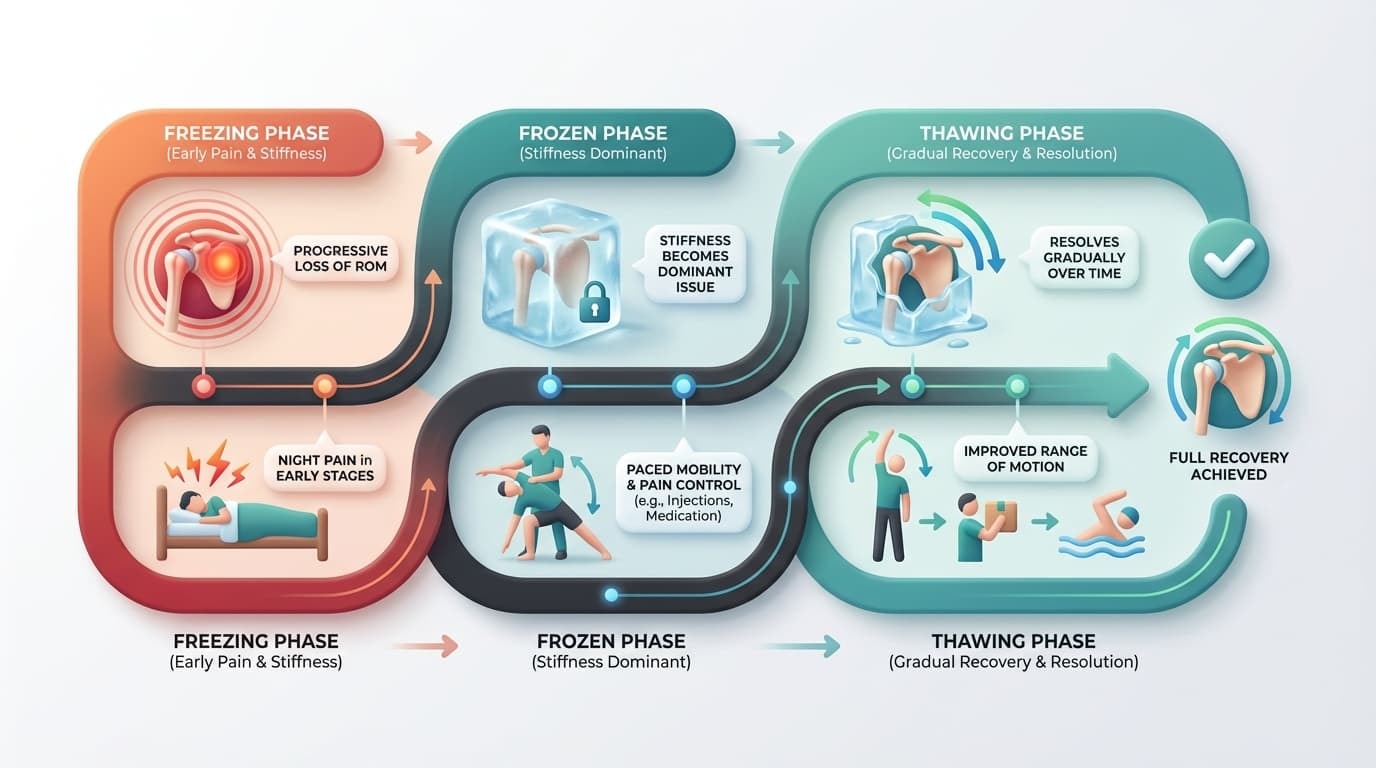
Frozen shoulder is very different from most other common shoulder injuries. Instead of sharp mechanical pain with lifting, the main issue becomes stiffness. The shoulder joint capsule thickens and tightens, limiting motion in every direction.
What Makes Frozen Shoulder Unique
Unlike many shoulder injuries, frozen shoulder restricts both active and passive movement. That means even if someone else tries to move your arm for you, it still will not go much farther. Pain is often worse early on, especially at night, and then stiffness becomes the dominant issue.
Typical features include:
-
Gradual onset without a major injury
-
Progressive loss of range of motion
-
Difficulty reaching overhead or behind your back
-
Night pain in the early stages
Do Injections Help?
A 2025 multisociety guideline reports that intra-articular corticosteroid injections can provide short-term relief, typically lasting from a few weeks to a few months. This temporary reduction in pain may help patients tolerate mobility work and rehabilitation more comfortably.
The same guideline notes that 20 mg of triamcinolone appears to be as effective as 40 mg for shoulder intra-articular or subacromial injections, suggesting higher doses may not always be necessary.
However, injections are not risk-free. Reported potential adverse effects include:
-
Increased blood glucose
-
Effects on bone mineral density
-
Possible cartilage impact
-
Risk of infection
-
Temporary adrenal suppression
Because frozen shoulder often resolves gradually over time, treatment usually focuses on paced mobility, pain control, and structured rehabilitation rather than aggressive stretching or repeated injections.
The goal is steady, controlled progress. Pushing too hard often increases irritation instead of improving motion.
Arthritis and Degenerative Shoulder Conditions
As we age, the shoulder joint naturally undergoes wear. Cartilage that cushions the joint surfaces gradually thins, and the smooth glide between the upper arm bone and the socket can become less efficient. This is how degenerative shoulder conditions develop.
Arthritis most commonly affects the glenohumeral joint or the acromioclavicular joint. Inflammatory conditions such as rheumatoid arthritis can also involve the shoulder, sometimes affecting both sides.
Common Symptoms
Degenerative shoulder conditions often present with:
-
Deep, aching shoulder pain that builds gradually
-
Stiffness after rest
-
Grinding or creaking sensations with movement
-
Reduced range of motion over time
Pain may worsen with sustained overhead activity or heavy lifting. Unlike acute injury, symptoms tend to progress slowly.
Imaging Does Not Always Tell the Whole Story
It is important to remember that imaging findings do not automatically explain symptoms. As discussed earlier in this guide, research shows that structural changes, such as rotator cuff tendinopathy or partial tears, can occur in people without shoulder pain.
The same principle applies to arthritis. Some individuals show clear degenerative changes on X-ray yet function well with minimal discomfort. Others have relatively modest imaging findings but significant symptoms.
Clinical evaluation and how your shoulder actually performs in daily life matter more than images alone.
Management Approach
Most degenerative shoulder conditions are managed conservatively at first. Treatment typically focuses on:
-
Strengthening surrounding muscles to offload the joint
-
Improving shoulder blade mechanics
-
Modifying aggravating activities
-
Using short-term pain relief strategies when appropriate
Surgical options such as shoulder replacement are generally reserved for severe arthritis with persistent pain and major functional limitation after structured conservative care.
The key message is this: degenerative does not mean hopeless. With the right plan, many people maintain strong, functional shoulders for years without needing surgery.
Less Common but Important Shoulder Injuries
Not every shoulder injury fits neatly into overuse, rotator cuff, instability, or arthritis categories. Some conditions are less common but still important to recognize, especially in athletes and high-impact environments.
Labral Tears
The glenoid labrum is a ring of cartilage that deepens the socket and helps stabilize the shoulder joint. A labral tear can occur from a fall, heavy lifting, repetitive overhead sports, or a previous shoulder dislocation.
Symptoms may include:
-
Deep, hard-to-pinpoint shoulder pain
-
Catching, clicking, or locking sensations
-
A feeling of instability during throwing or pressing movements
Certain types, such as SLAP tears, are more common among overhead athletes, such as baseball or volleyball players.
AC Joint Injuries
The acromioclavicular joint sits at the top of the shoulder, where the collarbone meets the shoulder blade. Direct impact to the shoulder, such as a fall or contact collision, can sprain or separate this joint.
Common signs include:
-
Pain directly on top of the shoulder
-
Tenderness when pressing the area
-
Pain when bringing the arm across the body
More severe separations may cause a visible bump at the end of the collarbone.
Biceps Tendon Injuries
The long head of the biceps tendon runs through the front of the shoulder. Repetitive strain or sudden loading can cause inflammation or tearing.
Typical symptoms include:
-
Front-of-shoulder pain with lifting
-
Discomfort during pulling or curling motions
-
A sudden bulge in the upper arm if the tendon fully tears
Many partial tears can be managed conservatively, depending on activity demands.
Fractures
Fractures of the clavicle, upper arm bone, or shoulder blade usually result from significant trauma such as falls, collisions, or vehicle accidents.
Warning signs include:
-
Severe pain after impact
-
Rapid swelling or bruising
-
Visible deformity
-
Inability to move the arm
These injuries require prompt medical evaluation to ensure proper alignment and healing.
While these conditions are less common than rotator cuff or overuse problems, recognizing their patterns early helps guide appropriate next steps and prevents long-term complications.
Safe First Steps: What to Do This Week
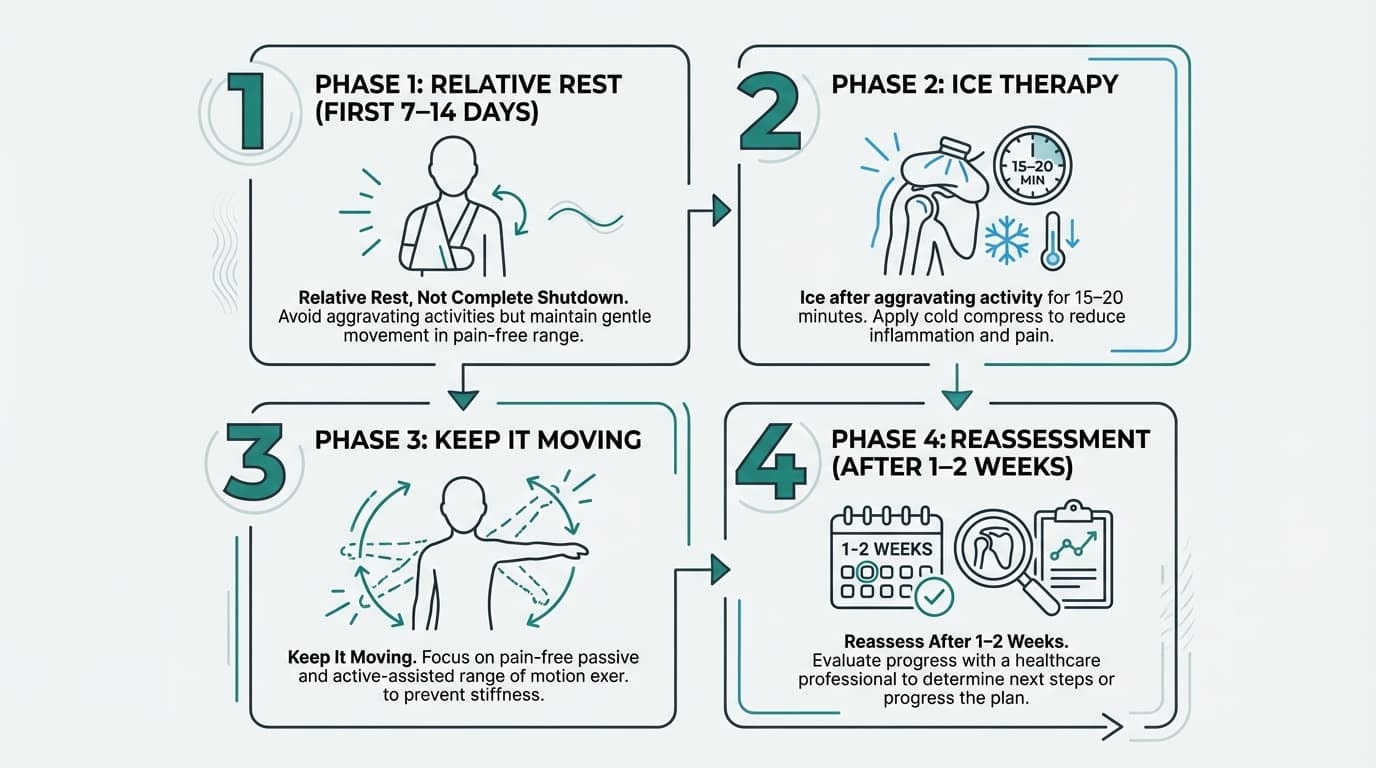
If your shoulder pain does not involve deformity, severe trauma, or neurological symptoms, the first 7–14 days should focus on calming irritation while keeping the joint moving safely.
1. Relative Rest, Not Complete Shutdown
Reduce movements that clearly aggravate symptoms:
-
Heavy overhead pressing
-
Repetitive throwing or serving
-
Deep bench pressing or dips
-
Sleeping directly on the painful side
At the same time, avoid full immobilization unless directed by a clinician. Gentle, pain-free movement keeps the shoulder joint from stiffening and prevents surrounding muscles from weakening.
During early return to activity, structured compression can provide proprioceptive feedback and joint support. Some athletes use external stabilization, such as the Anaconda Shoulder Brace, while rebuilding strength to help reduce the risk of re-aggravation. It should support your recovery process, not replace progressive strengthening and mobility work.
2. Calm Symptoms
-
Ice after aggravating activity for 15–20 minutes
-
Heat for muscle tightness if it feels better
-
Over-the-counter pain relief is appropriate for you
The goal is symptom control, so you can move better, not masking pain so you can train harder.
3. Keep It Moving
Start with gentle mobility:
-
Pendulum swings
-
Assisted arm lifts within a comfortable range
-
Light wall slides
Stop before sharp or catching pain. Consistency beats intensity.
4. Reassess After 1–2 Weeks
If pain is improving and range of motion is returning, gradually rebuild load.
If symptoms are unchanged or worsening, schedule a professional evaluation.
Most shoulder injuries respond well to smart early decisions. The key this week is simple: reduce irritation, maintain motion, and build back up deliberately.
When to Seek Professional Help for a Shoulder Injury
Most shoulder injuries improve with time, smart load management, and structured rehab. But there are moments when pushing through is not a strength. It is a risk.
If your shoulder pain is not following a steady improvement pattern, that is your first signal to pause and reassess.
Seek Prompt Evaluation If You Notice:
-
You cannot lift your arm after an injury
-
Pain wakes you every night and is not easing
-
Weakness is getting worse, not better
-
The shoulder feels unstable or like it may slip out
-
Numbness or tingling travels down the arm
-
Swelling, redness, fever, or visible deformity
These are not “train through it” signs. They are assessment signs.
When Pain Persists Beyond 2–3 Weeks
If your shoulder injury is not clearly improving after a few weeks of smart modification, it is time for professional input. A proper evaluation can clarify whether you are dealing with:
-
A significant rotator cuff tear
-
Shoulder instability
-
Frozen shoulder
-
Arthritis progression
-
A labral injury
Getting clarity early prevents months of frustration.
A Smart Conversation About Surgery
Surgery is sometimes necessary. But it should be a deliberate decision, not a rushed reaction to pain.
A 2024 study on rotator cuff repair reported an overall complication rate of 17.3%, with 20.3% in mini-open repairs and 13.8% in arthroscopic procedures. That does not mean surgery is unsafe. It means it carries real considerations.
A 2022 BMJ analysis of shoulder arthroscopy found:
-
90-day adverse events occurred in about 1 in 81 patients
-
Pneumonia occurred in 1 in 303
-
Pulmonary embolism occurred in 1 in 1428
These risks are relatively low, but they are not zero. Surgery can be life-changing in the right situation. It can also be avoided in many cases with structured rehabilitation.
The Bigger Picture
Most shoulder injuries respond to conservative treatment. Surgery is typically considered when:
-
There is a large acute tear with significant weakness
-
Instability keeps recurring
-
Pain and dysfunction persist despite months of high-quality rehab
The goal is not to avoid surgery at all costs. The goal is to make an informed decision.
If something feels off, trust that instinct. Getting evaluated does not commit you to an operation. It gives you clarity.
And clarity is what allows you to move forward with confidence.
Imaging Myths: When Scans Help and When They Confuse
When shoulder pain starts, many athletes assume the next step is a scan. MRI. Ultrasound. X-ray. It feels logical. Find the damage, fix the injury.
But imaging does not always tell the full story.
A 2025 population-based ultrasound study found that many adults had rotator cuff changes despite having no shoulder pain. In other words, structural findings on a scan do not automatically explain your injury. Imaging can show wear, thickening, or partial tears in the tendons even when the shoulder functions normally.
A 2022 systematic review of shoulder pain research also highlighted how widely prevalence data varies depending on how studies define injury and measure symptoms. Estimates shift based on age, activity level, and case definitions. This evidence heterogeneity matters. It means scans must be interpreted in context, not in isolation.
When Imaging Helps
Imaging becomes more useful when:
-
There is significant trauma
-
Weakness suggests a large tear
-
Instability episodes are recurring
-
Symptoms fail to improve with appropriate medical care
-
Surgical planning is being considered
In these cases, scans can guide treatment includes decisions about rehab progression or whether surgical referral is appropriate.
When Imaging Creates Confusion
Imaging too early can sometimes increase anxiety. Seeing words like “tear” or “degeneration” on a report can make an athlete assume severe injury, even when symptoms are mild.
In sports med settings, clinicians often rely first on clinical examination and functional testing of the shoulder and arm. The goal is to understand how the shoulder performs, not just what it looks like on a screen.
The Right Order
For most non-traumatic shoulder injury patterns, the smarter sequence is:
-
Clinical evaluation
-
Structured rehab
-
Reassessment
-
Imaging only if recovery stalls
Good medical care matches the scan to the situation. Imaging is a tool. It is not a diagnosis by itself.
Understanding this helps reduce panic and keeps the focus where it belongs: restoring strength, control, and confident movement in your arm.
Final Thoughts: Most Shoulder Injuries Improve With the Right Plan
Shoulder pain can feel overwhelming, especially when you read about tears, dislocations, and surgery online. But here is the reality: most shoulder injuries improve with the right plan.
Early pattern recognition changes everything. Understanding whether your issue is overuse, instability, stiffness, or irritation of the rotator cuff makes your next step clearer. Conservative care, guided strength work, smart activity modification, and patience solve far more problems than people expect.
Intelligent training matters. Reducing load does not mean stopping completely. It means adjusting, rebuilding, and progressing with intention. Shoulders respond well to consistent, progressive rehab when you respect the signals they give you.
At Anaconda Fightwear, we believe training should feel strong, not uncertain. With early pattern recognition, smart load management, and structured support when needed, most shoulder injuries improve without surgery.
Frequently Asked Questions
Still unsure what your shoulder is telling you? Here are clear, direct answers to the most common questions we hear from athletes.
How do I tell the difference between a simple shoulder strain and a rotator cuff tear?
A simple strain usually causes soreness and mild weakness, but you can still move your shoulder through most of its range of motion. A rotator cuff tear often creates true weakness, especially with lifting the arm bone away from the body or with external rotation. If your shoulder cannot lift the arm overhead, or weakness does not improve after 1–2 weeks, a clinical assessment with a physical examination is important. Acute shoulder injuries from direct trauma or a fall on an outstretched arm deserve earlier evaluation, particularly in contact sports or young male athletes.
Can imaging like MRI or ultrasound show shoulder damage even if I do not feel much pain?
Yes. Imaging can show changes in the rotator cuff tendons, supraspinatus tendon, glenohumeral joint, or even the superior labrum even when shoulder function feels normal. Many people have rotator cuff tendinopathy or minor soft tissue structures changes without symptoms. Family physicians and orthopaedic surgeons emphasize that scans must match your physical examination and clinical tests. Shoulder problems should be treated based on how the shoulder moves and performs, not just what appears on imaging.
Is it safe to keep working out or playing sports with shoulder pain?
It depends on the type of shoulder pain. Light, pain free movement that does not increase acute pain is usually safe while you begin conservative treatment. Modifying overhead work, reducing handball throwing load, or avoiding deep internal rotation and aggressive external rotation can help reduce pain. However, pushing through impingement syndrome, recurrent instability, or pain after a dislocated shoulder can worsen injury to the shoulder socket or joint capsule. If pain increases or shoulder function declines, start physical therapy or seek medical care.
How long do common shoulder injuries take to heal?
Most common injuries follow predictable timelines. Mild strains often improve in 2–4 weeks. Overuse patterns like rotator cuff tendinopathy or impingement syndrome may take 4–8 weeks with structured rehab. Partial tears, biceps tendon tears, or AC joint irritation may take several months. Adhesive capsulitis, also called frozen shoulder, can last much longer but still improves with conservative treatment. Healing depends on your age, consistency with stretching exercises, and how well you protect the shoulder during recovery.
Will I definitely need surgery if I have a rotator cuff tear or labral tear?
No. Many rotator cuff tears and superior labrum injuries respond well to conservative treatment and do not require surgery. Surgical intervention is usually considered only when shoulder function remains limited, chronic pain continues despite proper rehab, or there is significant structural damage. Orthopaedic surgeons and elbow surgeons typically recommend exhausting non-operative treatment options first. Orthopedic surgery is reserved for cases where recovery stalls or recurrent instability prevents safe return to sport.













