

You go to reach for your sports bra after a workout and boom! That sharp pull in your shoulder stops you mid-movement. Or maybe it’s not dramatic at all. Just that annoying ache that won’t quit after a long day at work or grinding through training.
If you’ve been Googling, “Causes of shoulder pain in females”, you’re being smart. Shoulder pain in women is incredibly common, and it doesn’t always mean the same thing.
As athletes (and as humans who just want to move without wincing), we know how frustrating it is when your shoulder won’t cooperate. At Anaconda, we’ve seen it on the mats, in the gym, and in everyday life.
Our goal here? Help you understand what’s likely going on, when self-care makes sense, and when you need urgent attention. And if your pain is musculoskeletal and training-related, our guide on training through a muscle strain safely can help you stay active while protecting your recover and our Anaconda Shoulder Brace is built to stabilize, compress, and protect so that you can move with confidence instead of fear.
Key Takeaways
-
Most shoulder pain in women comes from muscles, tendons, and joints—conditions such as rotator cuff irritation, bursitis, or frozen shoulder. With proper care, many of these improve over weeks to months.
-
Women report shoulder pain more often than men. Frozen shoulder, in particular, is more common between ages 40 and 60 and is strongly linked to diabetes and thyroid conditions.
-
There are female-specific triggers we see all the time: long hours at a desk, carrying heavy bags on one side, breast weight and bra straps altering posture, hormonal stiffness during perimenopause, and changes after breast cancer surgery.
-
Left shoulder pain plus chest pain, shortness of breath, sweating, or nausea? That’s emergency territory. Right shoulder pain after fatty meals may point toward gallbladder issues. Don’t ignore red flags.
Your Shoulder Isn’t “Just a Joint”; It’s a Moving Machine
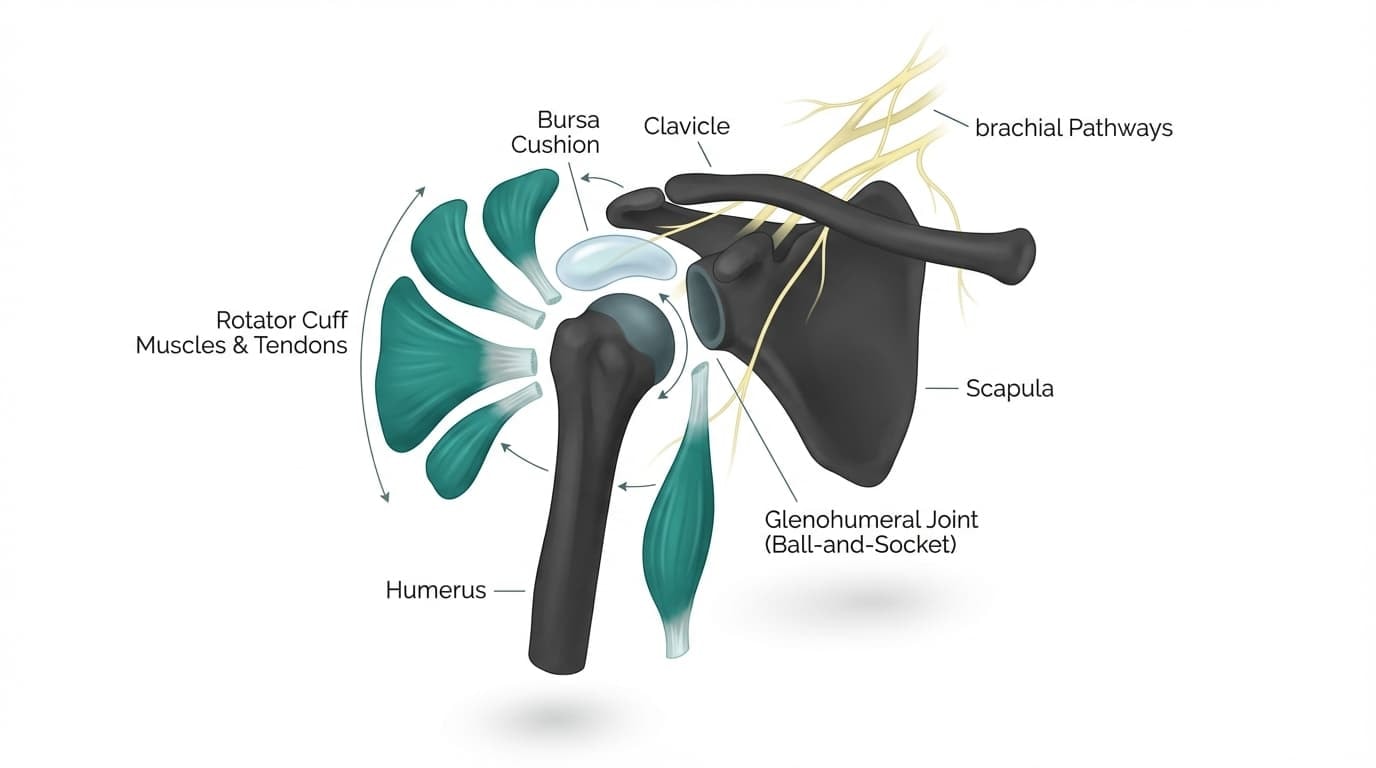
Your shoulder isn’t one simple hinge. It’s a team effort.
You’ve got:
-
The ball-and-socket joint (where your upper arm bone meets your shoulder blade)
-
The rotator cuff shoulder muscles and tendons that keep the ball centered
-
The bursa, which acts like a tiny cushion to reduce friction
-
The collarbone and shoulder blade are constantly coordinating movement
-
Nerves running down from your neck
All of that has to work together every time you:
-
Reach overhead
-
Throw a punch
-
Lift a child
-
Carry groceries
-
Fasten a bra behind your back
-
Sleep on your side
That’s a lot of responsibility for one region of the body.
The shoulder is designed for mobility over stability. It moves more than almost any other joint, but that freedom makes it vulnerable. If one muscle weakens, one tendon inflames, or posture shifts slightly, the whole system feels it.
So when something feels “off,” it’s rarely random. It’s usually your body telling you that one part of the moving machine is under strain.
Sometimes that strain is minor and manageable.
Sometimes it’s inflammatory.
Sometimes it’s stiffness locking the joint down.
And sometimes, though less commonly, the pain isn’t even coming from the shoulder at all.
That’s why we don’t brush off shoulder pain. And we don’t panic either. With the help of clinicians, we assess it calmly, informatively, and methodically.
Rapid Safety Check: When Shoulder Pain in a Woman Is an Emergency
Before we go any further, let’s slow this down for a second.
Most of the causes of shoulder pain in females are muscular and manageable. But there are situations where shoulder pain is your body waving a red flag, and those are the ones you never try to “push through.”
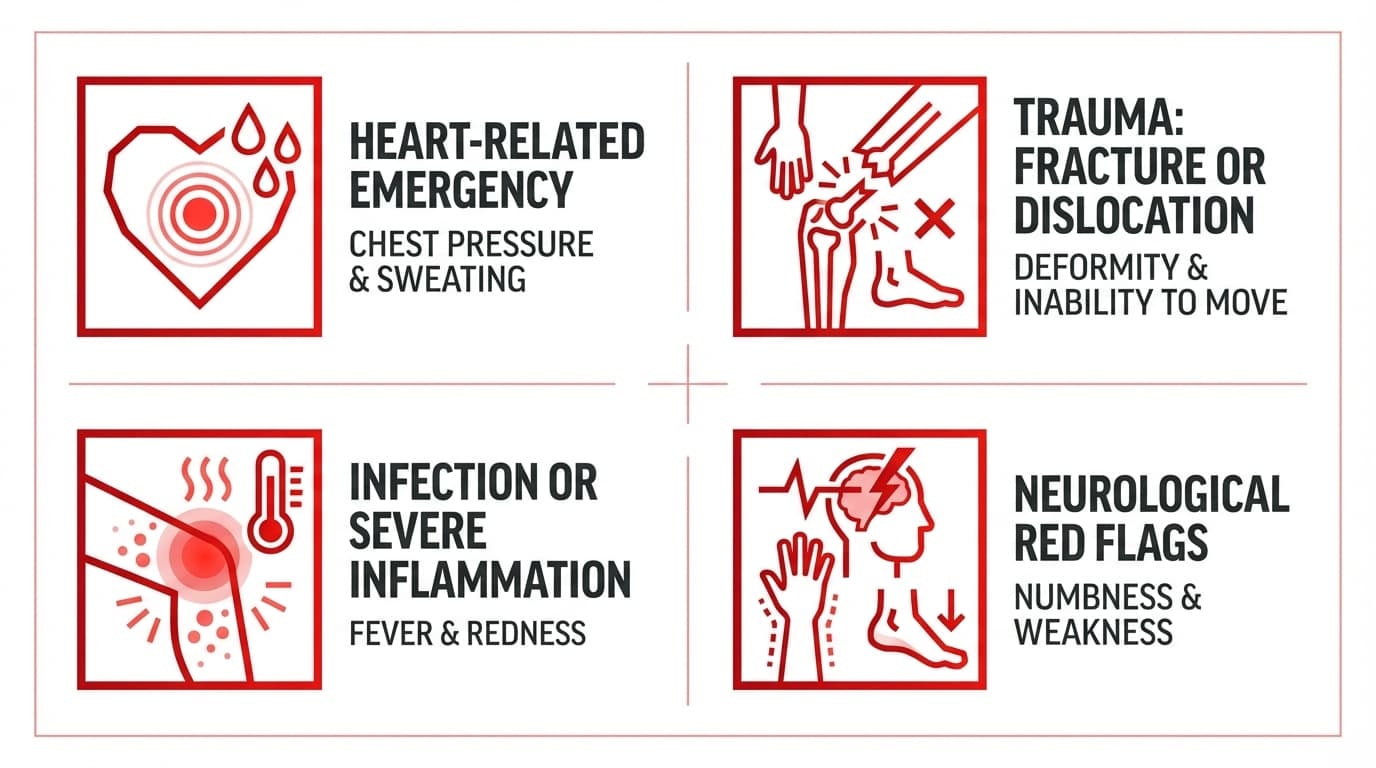
Possible Heart-Related Emergency (Call Emergency Services Immediately)
Women’s heart attack symptoms can look different. They can be subtle. And shoulder pain is one of them.
Call emergency services right away if you have:
-
New left shoulder, arm, or upper back pain with chest pressure or tightness
-
Shortness of breath
-
Sweating, nausea, or feeling lightheaded
-
Unusual extreme fatigue
-
Jaw pain or pain radiating down the arm
-
A feeling that “something isn’t right” along with shoulder discomfort
The American Heart Association emphasizes that women may not always have dramatic chest pain. Sometimes it’s shoulder or back pain with other subtle symptoms.
What to do:
Do not drive yourself. Call emergency services even if you’re unsure. It’s always better to be safe.
Trauma: Possible Fracture or Dislocation
If your shoulder pain started after a fall, car accident, or direct impact, pay attention.
Seek urgent care immediately if you notice:
-
Severe pain right after an injury
-
Visible deformity or your shoulder looks “out of place.”
-
Inability to move the arm at all
-
A loud “pop” followed by weakness
-
Swelling that rapidly worsens
What to do:
Immobilize the arm. Avoid trying to “pop it back in.” Go to the emergency room.
Infection or Severe Inflammation
This one is less common but still serious.
Watch for:
-
Shoulder pain with fever
-
Redness or warmth over the joint
-
Feeling suddenly very unwell
-
Recent injection, surgery, or systemic infection
What to do:
Contact your doctor immediately or go to an urgent care center. Joint infections require fast treatment.
Neurological Red Flags
Sometimes, shoulder pain actually comes from the neck or spinal nerves.
Urgent signs include:
-
Rapidly worsening numbness or tingling
-
Weakness spreading down the arm
-
Loss of bladder or bowel control with neck pain (rare but serious)
What to do:
Seek emergency evaluation.
Common Muscular and Joint Causes of Shoulder Pain in Females

Here’s the reassuring part. Most causes of shoulder pain in women are due to muscles, tendons, and joints. Not organs. Not emergencies. Just structures that have been overloaded, irritated, or inflamed.
Rotator Cuff Tendinitis and Partial Tears
Your rotator cuff is like your shoulder’s pit crew. Four muscles and their tendons work together to keep the ball of your shoulder joint centered and stable every time you lift, punch, reach, or carry.
When they get irritated or partially torn, you’ll usually feel:
-
A dull ache on the top or side of the shoulder
-
Pain lifting overhead
-
Pain reaching behind your back (yes, fastening a bra becomes a struggle)
-
Night pain when lying on that side
-
Weakness when lifting objects
Rotator cuff tendinitis is one of the most common causes of shoulder pain in both men and women.
What’s more, ultrasound studies show that about 34% of people without any pain have rotator cuff changes on imaging. That means scans don’t automatically equal surgery. Pain and function matter more than imaging alone.
Shoulder Impingement and Bursitis
This one feels like a “pinch.”
The rotator cuff tendons pass under a bony arch called the acromion. When mechanics are off, tight muscles, poor posture, and repetitive shoulder movements overhead can compress the tendons, causing shoulder impingement.
The nearby fluid-filled sac (bursa) can become inflamed as well. That’s shoulder bursitis.
You might notice:
-
Sharp pain between 60 and 120 degrees when lifting your arm
-
Pain when blow-drying hair or reaching overhead
-
Increased discomfort after laptop work
-
Tenderness on the outer shoulder
The good news? This is often very responsive to rest, mobility work, strengthening, and reducing mechanical overload.
Frozen Shoulder (Adhesive Capsulitis)
This one deserves special respect.
Frozen shoulder affects about 2–5% of people, but women account for roughly 67% of cases, most commonly between the ages 40 and 60.
If you’re in that age range and noticing increasing stiffness without a clear injury, this should be on your radar.
Risk factors include diabetes (which doubles the risk), thyroid disorders, and perimenopausal hormonal shifts.
This condition is frustrating. It takes time. But it usually resolves with guided care and patience.
Degenerative Conditions (Osteoarthritis & AC Joint Arthritis)
Over time, cartilage can wear down causing degenerative changes in the joint.
You may notice:
-
Grinding or crunching
-
Morning stiffness
-
Pain when crossing your arm across your body
-
Gradual worsening over months or years
Rheumatoid arthritis, an autoimmune condition more common in womenm can also inflame the shoulder joint. This is less about acute injury or sudden shoulder pain and more about long-term management.
Muscle Strain and Postural Overload
Sometimes it’s not dramatic. It’s cumulative.
Common patterns we see:
-
Carrying heavy handbags
-
Long hours hunched at a laptop
-
Rounded shoulders and forward head posture
-
Holding a child
These often causes tension radiating from the shoulder blade into the upper arm. It feels tight. Achy. Sometimes burning.
This is where smart strengthening, posture awareness, and supportive compression during activity can really help reduce strain.
Neck, Nerve, and Upper-Back Causes That Feel Like Shoulder Pain
Here’s something we tell athletes all the time.
Just because it hurts in your shoulder doesn’t mean the shoulder is the real problem.
Some women experience pain that actually starts in the neck or upper spine and radiates into the shoulder.
Understanding this difference matters. Because treating a nerve problem like a rotator cuff injuries won’t fix it.
Cervical Radiculopathy (Pinched Nerve in the Neck)
Your neck houses nerve roots that travel down into your shoulder and arm. When something compresses one of those nerves, like a disc bulge, arthritis, or bone spur, the pain can shoot into the shoulder.
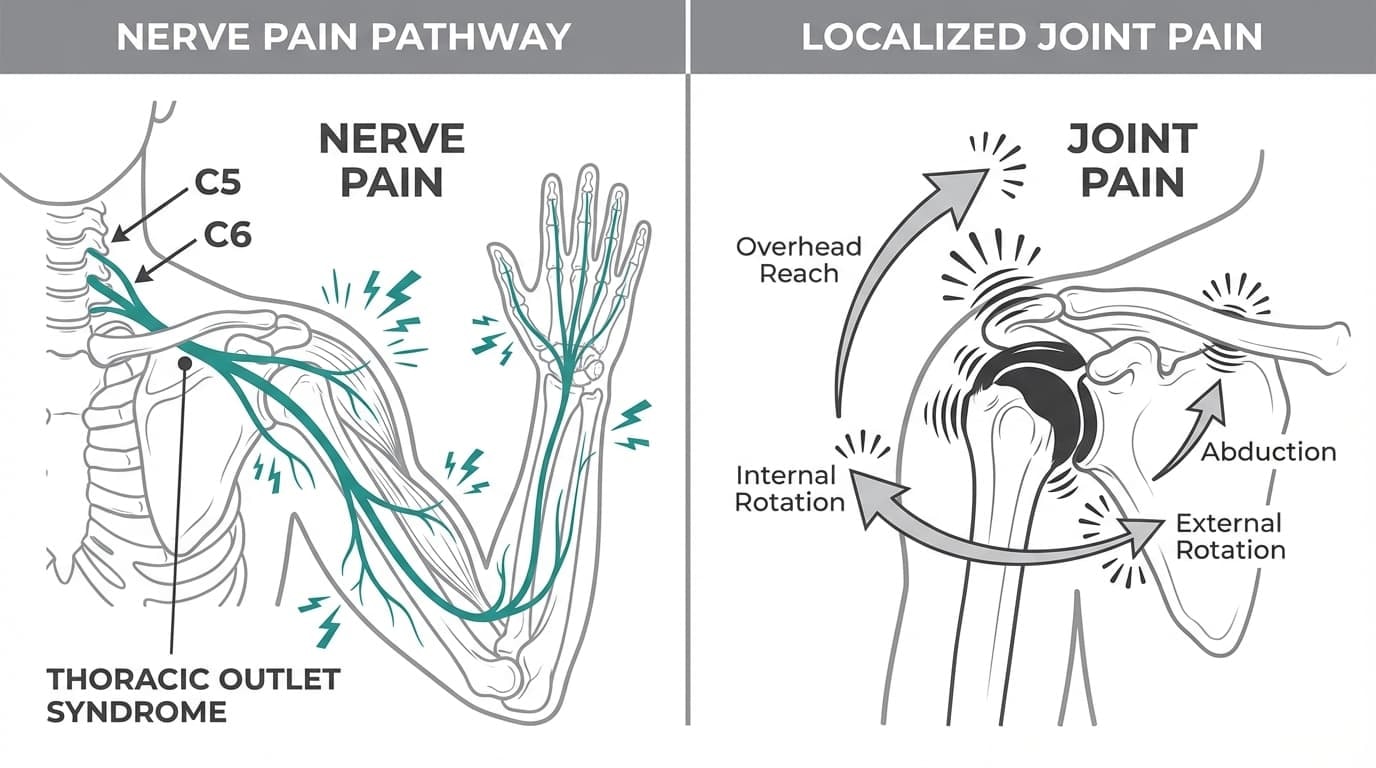
In cervical radiculopathy, commonly affected nerves are C5 and C6.
What it feels like:
-
Pain that starts in the neck and travels into the shoulder
-
Shooting or electric pain down the arm
-
Tingling or numbness in the forearm or hand
-
Weakness in the arm
-
Symptoms that worsen when you move your neck (not just your shoulder)
Here’s the key difference:
Joint pain usually stays in the shoulder and worsens with arm movement. Nerve pain often follows a line from the neck into the arm and worsens with neck movement.
If you’ve ever felt that lightning-bolt sensation when turning your head, that’s a clue.
And if you’re dropping objects or feeling true weakness (not just soreness), that’s not a “stretch it out” situation. That’s the clue to speak with your doctor immediately.
Thoracic Outlet Syndrome (TOS)
This one is more common in women than most people realize.
Thoracic outlet syndrome happens when nerves or blood vessels get compressed between your collarbone and first rib.
We see this more often in:
-
Women with sloped shoulders
-
Those who carry heavy handbags on one side
-
People with poor posture
-
Athletes doing repetitive overhead work
Symptoms can include:
-
Heaviness in the arm
-
Fatigue when holding the arm up
-
Tingling in the hand
-
Arm feeling cold or changing color
-
Symptoms worsen with overhead posture or certain bra straps
Rather than a sharp joint pain, it feels like your arm just doesn’t have endurance…like something’s being squeezed.
Again, this condition needs a proper assessment by a medical professional. Self-diagnosing TOS can get tricky.
Brachial Plexus Irritation
The brachial plexus is a network of nerves that runs from your neck through your shoulder.
In brachial plexus irritation, it can get irritated by:
-
Whiplash
-
Sudden pulling injuries
-
Repetitive strain
-
Swimming
-
Overhead training
-
Even sleeping awkwardly
Symptoms may include:
-
Burning pain around the shoulder
-
Radiating discomfort into the arm
-
Weakness
-
Numbness
Again, the pattern matters.
If the pain travels and changes with neck posture, think nerve. If it stays localized and hurts with arm motion, think joint or tendon.
And we’ll say this gently but clearly.
If you’re noticing persistent numbness, progressive weakness, coordination issues, or dropping objects, don’t just rely on YouTube stretches. Get evaluated by your doctor.
At Anaconda, we believe in training smart. Nerves are not something you “push through.”
Visceral (Organ) Causes of Right Shoulder Pain in Females
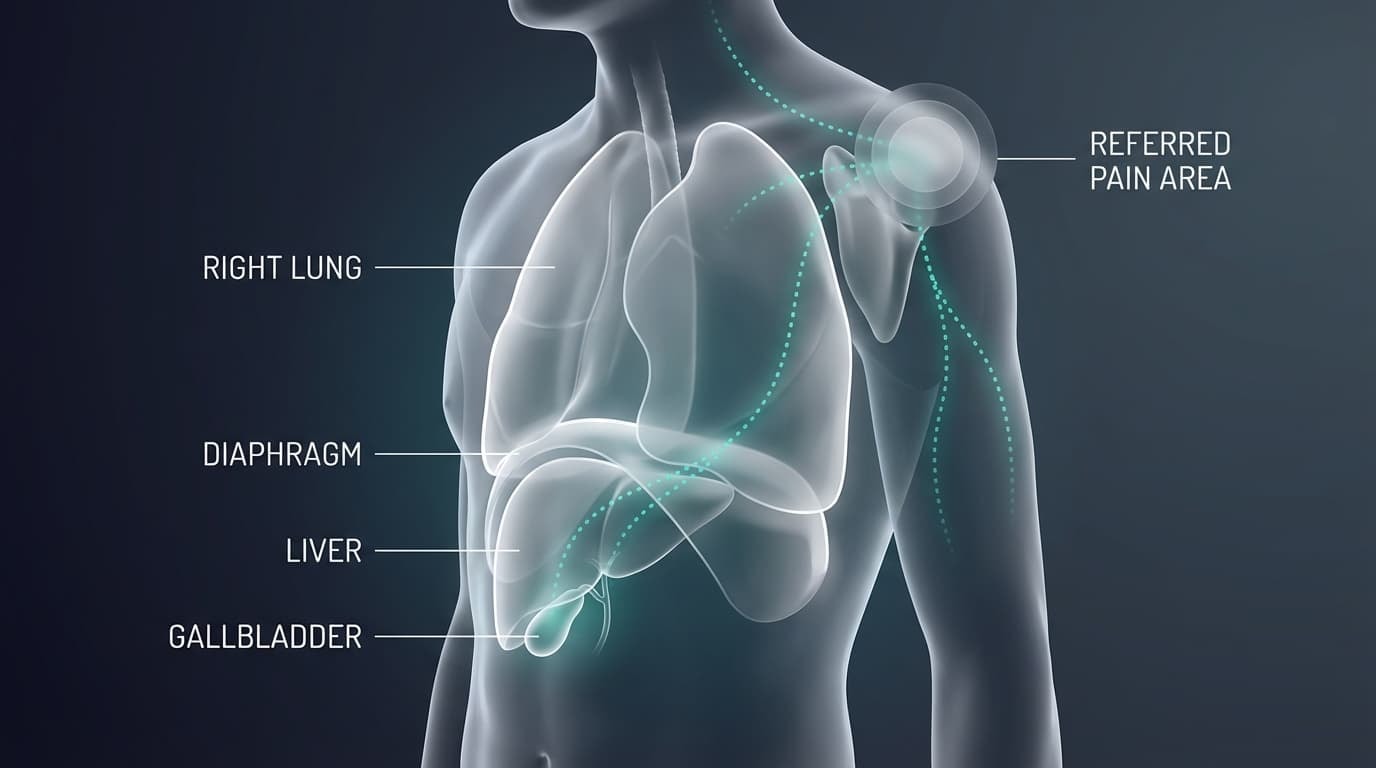
Right shoulder pain can sometimes be the body’s weird way of saying, “Hey, check your organs.”
The brain interprets signals from organs and sometimes sends that signal to the shoulder because they share nerve pathways.
Gallbladder-Related Pain
Gallbladder-related pain is one of the most classic patterns.
Gallbladder issues can cause:
-
Right shoulder or shoulder blade pain
-
Upper right abdominal pain
-
Nausea after fatty meals
-
Pain that worsens in the evening
It’s particularly common in midlife women.
The key pattern is that pain is not triggered by arm movement, but by eating.
If you notice right shoulder pain repeatedly after meals, especially greasy or fatty foods, book a medical evaluation.
Liver Conditions
Liver-related pain may cause vague discomfort in the upper abdomen and right shoulder.
Watch for:
-
Yellowing of eyes or skin
-
Dark urine
-
Unexplained fatigue
-
Abdominal swelling
These symptoms are not something to ignore.
Lung and Diaphragm Causes
Conditions like:
-
Pneumonia
-
Pleurisy (inflammation of the lung lining)
-
Lung masses
Can refer pain to the right shoulder.
Usually accompanied by:
-
Cough
-
Shortness of breath
-
Pain with deep breathing
-
Fever
All in all, if your right shoulder pain appears with fever, unexplained weight loss, persistent cough, abdominal pain, or feeling generally unwell, seek medical care.
Don’t self-diagnose.
Female Life-Stage and Surgery-Related Causes of Shoulder Pain
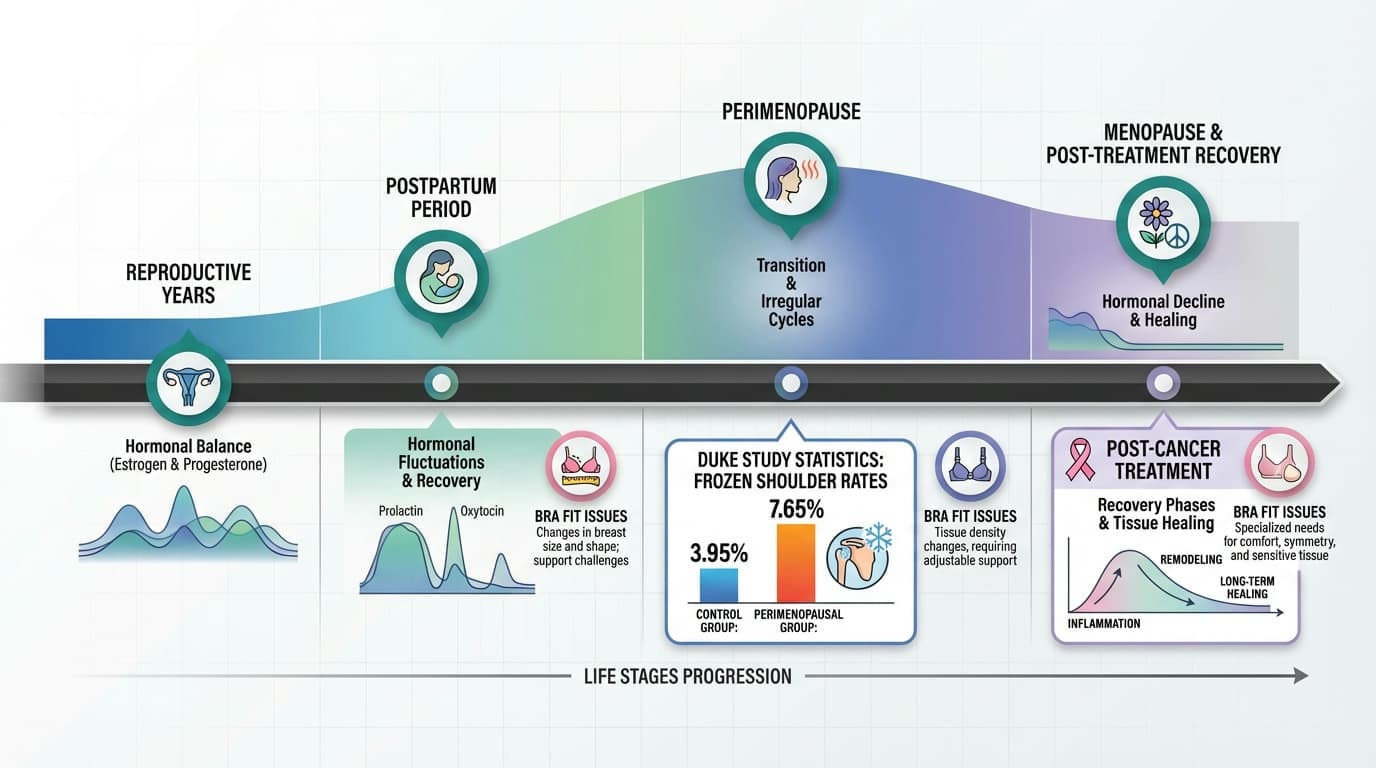
When we talk about causes of shoulder pain in women, we can’t ignore biology.
Hormones shift. Life stages change. Surgeries happen. And all of that can impact how your shoulder feels and functions.
Perimenopause and Menopause
The 40s and 50s can feel like a plot twist for your joints.
As estrogen declines:
-
Tendon integrity can decrease
-
Bone density changes
-
Joint mechanics shift
-
Inflammation patterns evolve
-
Frozen shoulder risk rises significantly
Frozen shoulder is notably more common during this phase of life.
A Duke Health retrospective study of nearly 2,000 postmenopausal women found:
-
3.95% of women on estrogen replacement developed frozen shoulder
-
7.65% of women not on estrogen did
That difference suggests estrogen loss may directly contribute to increased shoulder stiffness during this transition.
Add in diabetes or thyroid conditions, which are already risk factors for frozen shoulder, and the likelihood increases.
So, if you’re between 40 and 60 and noticing gradual stiffness and night pain, you’re not imagining it. Hormones matter.
Postpartum and Caregiving Patterns
New motherhood is beautiful, and biomechanically brutal.
Common patterns include:
-
Breastfeeding with rounded shoulders
-
Looking down for long periods
-
Rocking and carrying infants
-
Lifting car seats repeatedly
-
Sleep deprivation affects tissue recovery
That constant forward posture loads the neck and upper back, which then feeds into the shoulder.
It often feels like:
-
Burning around the shoulder blade
-
Deep ache in the upper arm
-
Tension that won’t fully release
It’s accumulated strain. And it’s incredibly common.
Bra Fit and Breast Size
This one doesn’t get talked about enough.
Heavy breasts or poor bra support can:
-
Increase the forward shoulder pull
-
Create chronic trapezius tension
-
Cause narrow straps to dig into the muscle
-
Lead to trigger points and radiating pain
Over time, that mechanical load can alter shoulder mechanics.
We understand how frustrating it is when something so daily contributes to discomfort. Small ergonomic changes can make a real difference.
Post–Breast Cancer Treatment Shoulder Pain
This deserves careful, respectful attention.
A 2015–2023 retrospective review of 773 women after mastectomy and reconstruction found that 24.8% experienced shoulder impairment that started around 244 days after surgery. They also found that it lasted for 293 days.
Common post-treatment issues include:
-
Scar tightness that limits overhead motion
-
Chest wall tenderness
-
Protective muscle guarding
-
Lymphedema-related heaviness
-
Adhesions affecting rotation and lifting
Early referral to oncology-focused physical therapy is crucial.
We say this gently. If you’ve gone through breast cancer treatment and your shoulder doesn’t feel the same, that is valid. And you deserve specialized care.
How Shoulder Pain in Women Is Diagnosed
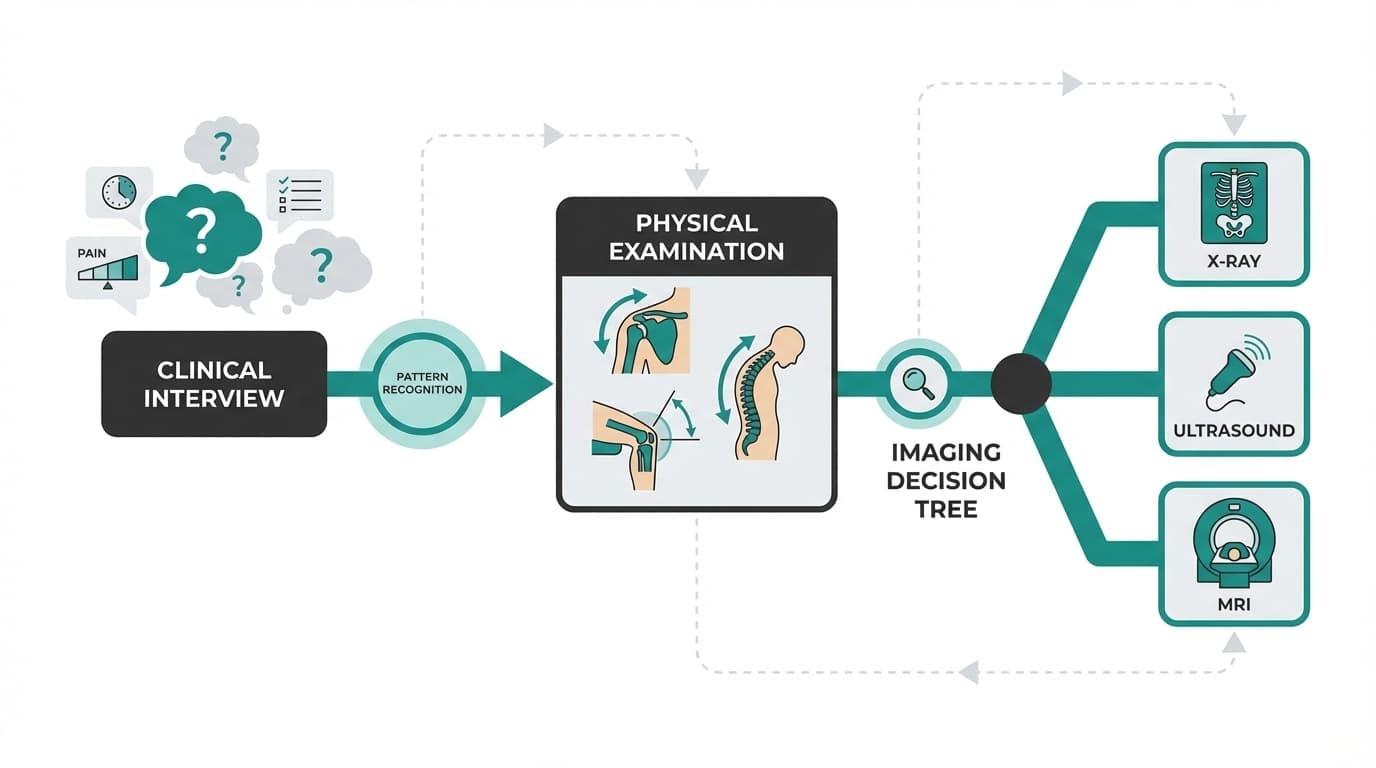
Diagnosis isn’t guesswork. It’s pattern recognition.
A good clinician will start with your story.
What a Clinician Will Ask
Expect questions about:
-
When did it start? Sudden injury or gradual?
-
Where exactly is the pain?
-
What movements make it worse?
-
Does it wake you at night?
-
Any chest, abdominal, fever, numbness, or weakness symptoms?
Your answers guide everything.
The Physical Examination
A proper exam usually includes:
-
Active and passive range of motion
-
Specific strength testing for each rotator cuff muscle
-
Impingement tests
-
Neck movement assessment
-
Neurological screening
Often, this exam alone provides clarity.
Imaging Tools
If the need pops up, doctors might recommend specific imaging to further identify the root cause. However, many shoulder pain cases are diagnosed without advanced imaging.

Blood tests may be ordered if infection, autoimmune disease, or organ disease is suspected.
Treatment Options for Shoulder Pain in Females
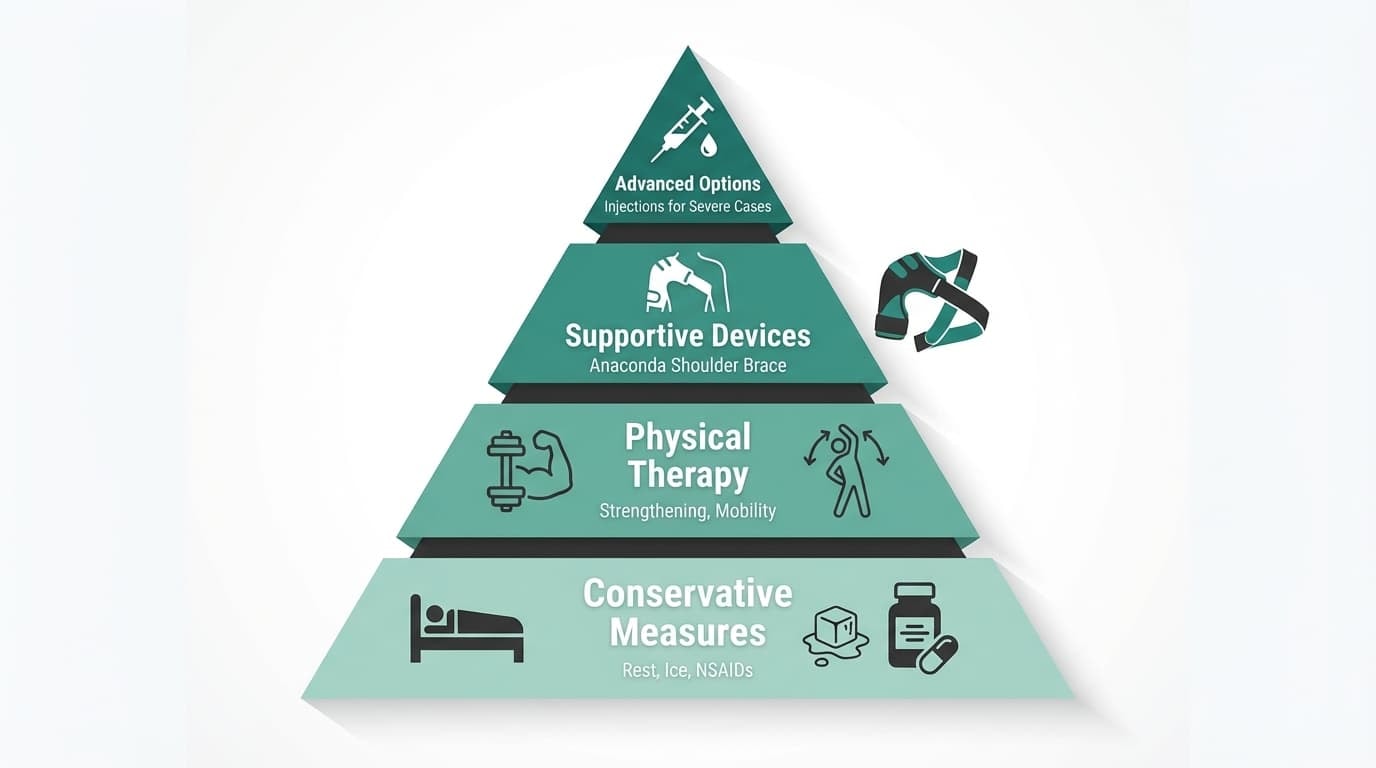
Now, for the encouraging news! Most women improve with structured non-surgical care.
Conservative Measures
First-line treatment often includes:
-
Relative rest (not total immobilization)
-
Ice for inflammation
-
Heat for muscle tension
-
Short-term nonsteroidal anti inflammatory drugs like ibuprofen or naproxen
-
Gentle mobility within pain-free range
Physical Therapy
Physical therapy is often the game-changer. PT focuses on:
-
Strengthening rotator cuff and scapular stabilizers
-
Posture retraining
-
Frozen shoulder mobility protocols
-
Neck treatment when needed
-
Postpartum and post-surgical programs
Many women see improvement within 6–12 weeks for common conditions.
Where the Anaconda Shoulder Brace Fits In
Here’s where we at Anaconda always emphasize balance.
A brace is not a replacement for medical care. It’s not a fix for nerve compression or organ-related pain.
But for mechanical shoulder strain, tendon irritation, and training-related instability, it can be a powerful support tool.
Our Shoulder Brace provides:
-
Targeted 3D compression to improve circulation
-
Stability without bulk
-
Gel padding for shock absorption
-
Secure dual straps to prevent shifting
-
Full mobility during training
That compression supports blood flow, helping oxygen and nutrients reach irritated tissue while reducing strain during activity.
We’ve seen athletes use it during rehab phases to:
-
Reduce discomfort during modified training
-
Protect healing tissue
-
Maintain confidence while rebuilding strength
Our promise is simple: support recovery without limiting performance.
Injection Options
If conservative care needs help:
-
Corticosteroid injections for bursitis or frozen shoulder flares
-
PRP (evidence still evolving)
These require individualized discussions with your provider.
Strong, Informed, and Back in Control
Shoulder pain can feel overwhelming, especially when you’re trying to balance work, family, training, and life. But most causes of shoulder pain in women are not catastrophic.
They’re mechanical. They’re hormonal. They’re posture-related. And they’re manageable.
The key is knowing the difference between something that needs emergency care or medical evaluation and something that needs smart self-care and structured support.
At Anaconda, we’ve lived through injuries that stopped us in our tracks. We understand what it feels like when your body won’t cooperate. That’s why we crafted the Anaconda Shoulder Brace to support your recovery.
If your shoulder pain falls into the common mechanical categories, tendon irritation, instability, or overload, the Anaconda Shoulder Brace is built to support you while you rebuild:
Over 300,000 athletes train with confidence using our brace because it supports recovery without slowing you down.
You don’t have to ignore pain.
You don’t have to panic either.
Train smart. Heal smart. Protect your progress.
FAQ: Women’s Shoulder Pain — Real Questions, Real Answers
Here at Anaconda, we believe informed athletes make stronger decisions. These are the questions we hear most often.
Can stress or anxiety really cause shoulder pain in women?
Yes, and it’s more common than people realize.
Stress triggers chronic tightening of the neck, shoulders, and upper back. The trapezius muscle (that big muscle from your neck to your shoulder blades) is especially reactive to emotional tension.
Combine that with lifestyle habits like long hours on a laptop and unmanaged stress and you’ve got a recipe for persistent aching, burning, and even tension headaches.
Movement breaks, relaxation techniques, breath work, and gentle stretching can help a lot.
But here’s the important part. If pain is one-sided, progressively worsening, or accompanied by weakness, get evaluated. Stress may contribute, but structural causes still need to be ruled out.
Why does my shoulder pain get worse at night?
Night pain is a classic feature of rotator cuff irritation.
When you lie on the affected side, irritated tendons and bursae get compressed against the bone. Even lying on your back can let the arm fall backward, stretching inflamed tissue.
Frozen shoulder is also notorious for intense night pain during its early “freezing” phase. Inflammatory arthritis can feel worse at rest or first thing in the morning, too.
For side sleepers, hug a pillow to prevent the top shoulder from collapsing forward. While for back sleepers, place a small pillow under the arm.
If night pain lasts more than 2 weeks or significantly disrupts sleep, book a clinician visit.
Sleep matters for healing.
Is shoulder pain during menopause normal?
It’s not inevitable, but it is more common.
Declining estrogen affects tendon integrity, joint stability and inflammation levels. Frozen shoulder risk increases during perimenopause. Research shows significantly higher rates in women during this transition.
Don’t brush off new shoulder symptoms as “just menopause.”
Mention them to your clinician, especially if you’re also experiencing hot flashes, sleep disruption, or metabolic changes. This is also the life stage where strength training, posture work, and metabolic health management become especially important.
How long should I try home treatment before getting an MRI?
For mild to moderate shoulder pain without trauma or red flags, many guidelines recommend trying 4–6 weeks of structured self-care or physical therapy. This is before jumping to advanced imaging like MRI.
Immediate imaging is more appropriate after:
-
Significant trauma
-
Sudden major weakness
-
Suspected full-thickness rotator cuff tear
-
Or when serious conditions need rapid exclusion
Remember: partial rotator cuff tears are common even in pain-free shoulders. Imaging must always be interpreted in conjunction with symptoms and physical exam findings.
Scans don’t treat pain. Smart care does.
Can I keep exercising if I have shoulder pain?
In many cases, yes, with modifications.
You can usually continue lower-body training, core work, and cardio that doesn’t aggravate the shoulder. You may need to temporarily avoid heavy pressing, overhead lifting, and high-load upper-body work.
During the first 1–2 weeks of new symptoms, respect irritation. As pain settles, gradually reintroduce movement.
A physical therapist or sports medicine clinician can build a “pain-respecting” plan.
And for mechanical instability or tendon irritation, supportive compression, like the Anaconda Shoulder Brace, can help protect the joint while you rebuild strength.













