

Shoulder pain causes elbow pain through a mechanism called referred pain, where irritation in the rotator cuff or cervical spine (neck) manifests as distal symptoms in the arm.
Clinical data indicates that approximately 30% of rotator cuff tendinopathy cases present with radiating pain that mimics local elbow conditions.
So, can shoulder pain cause elbow pain?
Yes. And it is more common than you think.
Referred pain occurs when the central nervous system misinterprets nociceptive signals from the shoulder joint, projecting the sensation solely to the elbow.
Shoulder-driven referral is distinct because the elbow joint itself remains mechanically sound despite the sensation of discomfort.
Many athletes who are dealing with shoulder pain are surprised when their elbow pain improves after the shoulder is addressed.
At Anaconda Fightwear, we work with over 300,000 athletes who train through shoulder pain and elbow pain every day. One of the most common questions we hear is whether elbow pain is really coming from the shoulder. In many cases, it is.
Key Takeaways
-
Elbow pain is not always an elbow problem. Pain felt at the elbow can originate from the shoulder or even the neck.
-
Movement patterns tell the real story. If shoulder motion triggers elbow pain, the shoulder may be the driver. If elbow movement alone hurts, it is more likely a local elbow issue.
-
Most cases improve without surgery. Early load management, smart strengthening, and structured rehab are effective for the majority of shoulder-to-elbow pain cases.
-
Red flags matter. Sudden weakness, trauma, swelling, chest symptoms, or spreading numbness require prompt medical evaluation.
Can Shoulder Pain Really Cause Elbow Pain?

Short answer? Yes.
Long answer? It happens more than most people realize.
If your elbow pain feels vague, deep, or like it runs down your upper arm, there is a strong chance the real issue is higher up. A rotator cuff injury can send pain signals down the upper arm and make it feel like the elbow joint is the problem, even when the elbow itself is fine.
This is called referred pain. Your nervous system is not always great at pinpointing where irritation starts. So shoulder irritation can show up as elbow pain.
A 2015 JOSPT clinical perspective reported that a significant proportion of rotator cuff tendinopathy cases present with pain radiating down the arm. That means this pattern is not rare. It is expected.
Then, in 2025, updated clinical practice guidelines highlighted an important point. When evaluating arm pain, clinicians must screen for cervical dysfunction and neurological symptoms. Why? Because shoulder and elbow conditions are often linked to the neck. What feels like tennis elbow could actually be part of a larger shoulder-and-elbow pattern.
Here is the good news.
Orthopedic data suggests that less than 10% of referral-based arm pain cases require surgical intervention.
Instead, physical therapists utilize structured load management and scapular strengthening to resolve symptoms in 12-16 weeks without operative measures.
True tennis elbow usually stays localized and involves the forearm muscles. But when pain tracks down the upper arm, changes with shoulder movement, or flares during overhead work, it points back to the shoulder.
The goal is not guessing. It is identifying the source. Once you understand whether it is a rotator cuff injury or another shoulder and elbow issue, pain relief becomes a plan, not a mystery.
Shoulder vs Neck vs Elbow: How to Tell Where Your Pain Is Coming From
When pain hits your arm, it is easy to assume the spot that hurts is the problem. But with the shoulder and elbow, that is not always true.
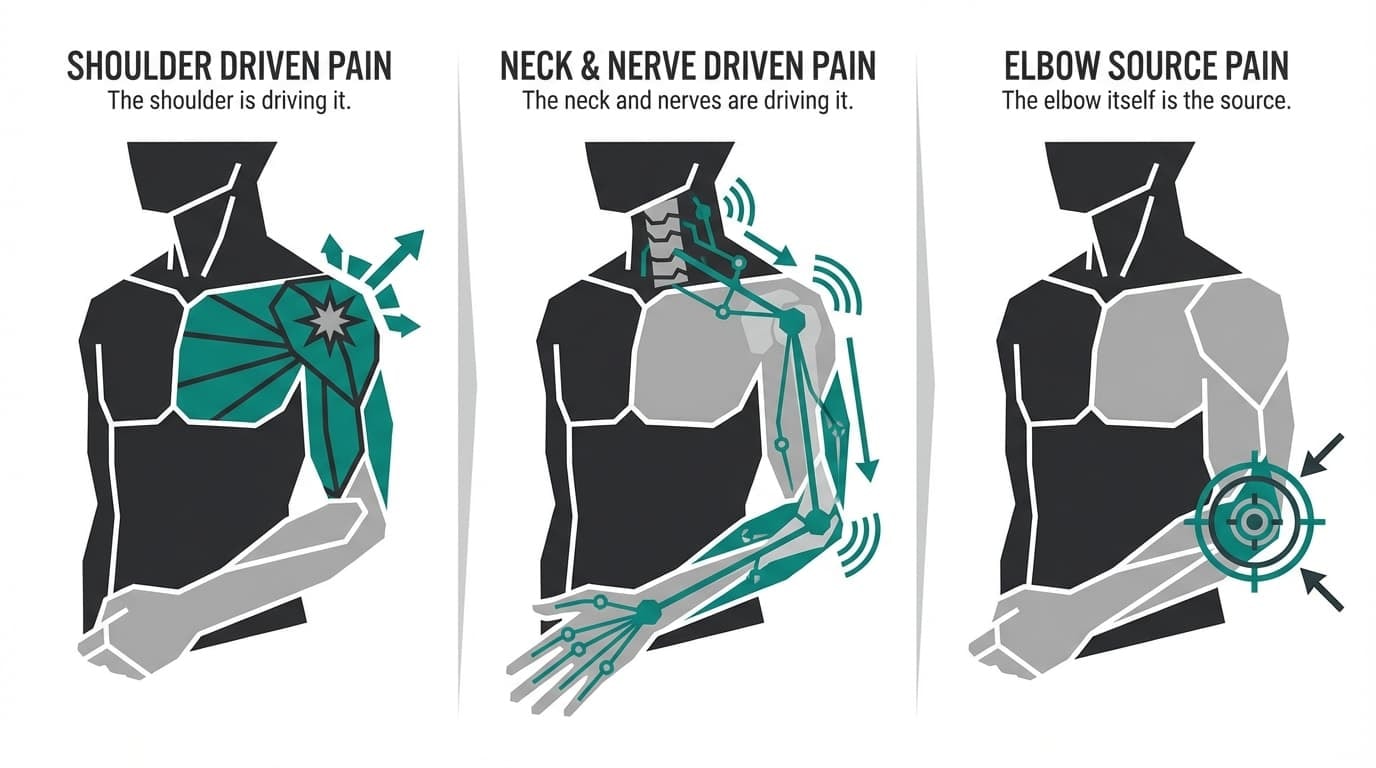
Pain in this area usually falls into one of three buckets:
-
The shoulder is driving it
-
The neck and nerves are driving it
-
The elbow itself is the source
Each one behaves differently. The way your pain responds to movement, posture, lifting, or even your sleeping position provides important clues.
In the next sections, we will break this down clearly. You will learn how to spot shoulder-driven referral, nerve-related symptoms, and true elbow conditions like tennis elbow. The goal is simple: help you narrow it down before you guess, Google, or panic.
Let’s sort it out.
Shoulder-Driven Pain That Radiates to the Elbow
Shoulder pain is common. A 2025 UK pathway analysis reported that approximately 2.4% of people attend primary care annually for shoulder pain, with higher reported rates in women. That tells us two things: this is widespread, and you are not alone.
When irritation develops in the shoulder joint, especially around the rotator cuff tendons or the biceps tendon, pain can travel down the upper arm and settle near the elbow. This is classic referred pain. The issue starts at the shoulder, but the discomfort shows up lower in the arm.
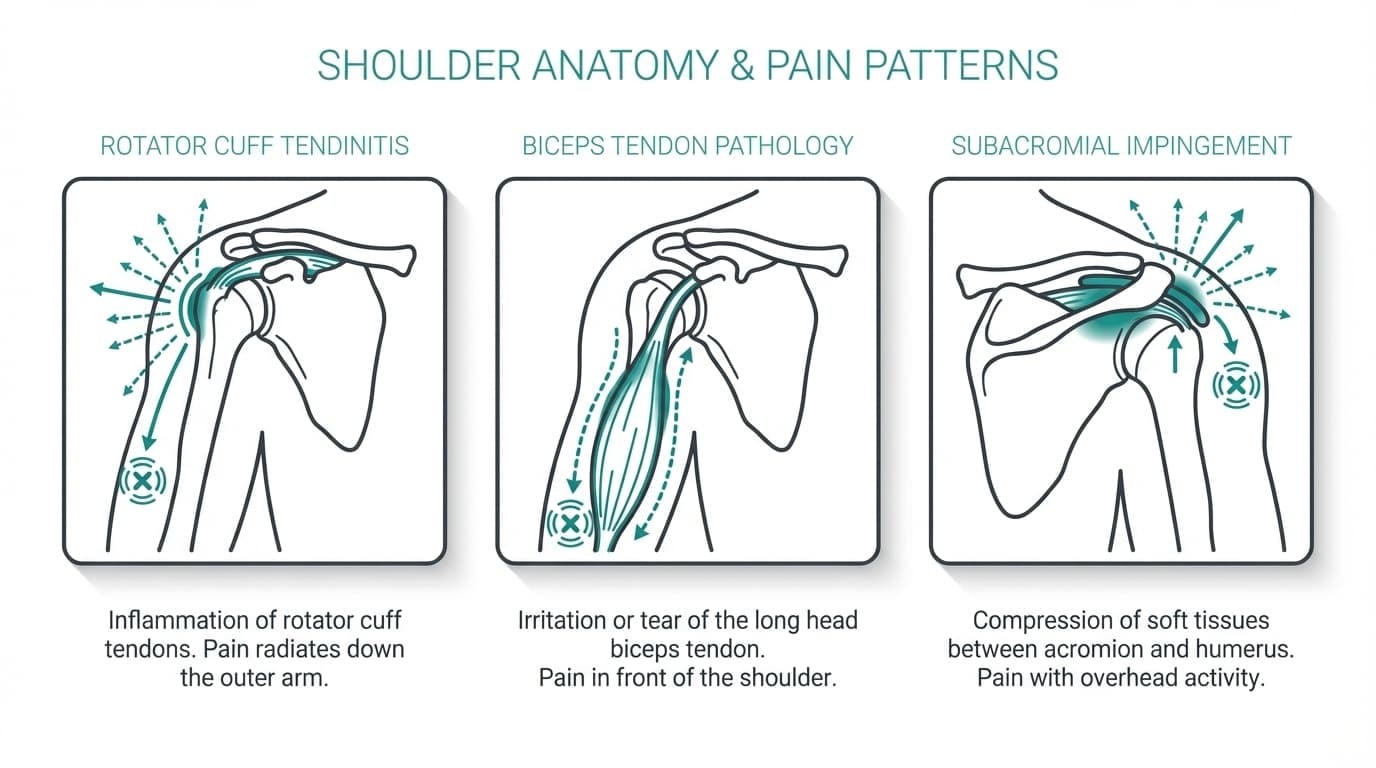
Common shoulder drivers include:
-
Rotator Cuff Tendinitis: Inflammation of the supraspinatus tendon often sends nociceptive signals down the lateral arm to the elbow.
-
Biceps Tendon Pathology: Proximal biceps irritation can radiate distally, mimicking antecubital (front of elbow) pain. > * Subacromial Impingement: Compression of soft tissue in the subacromial space creates a deep, aching referral pattern often felt at the mid-humerus and elbow.
In these cases, lifting the arm overhead, reaching behind your back, or rotating the shoulder tends to reproduce symptoms. The upper arm feels sore, sometimes deep and aching, and elbow stiffness can develop secondarily from guarding or reduced movement. Direct pressure on the elbow joint often does not trigger sharp pain the way true elbow injuries do.
Most shoulder and elbow conditions in this category respond well to conservative care. Activity modification, structured physical therapy, and progressive strengthening of the rotator cuff muscles are typically first-line strategies. Severe arthritis or inflammatory conditions, such as rheumatoid arthritis, are less common causes but should be ruled out if symptoms are persistent or systemic.
During this early recovery phase, some athletes choose external support to reduce joint strain while continuing light training. A structured brace, like the Anaconda Shoulder Brace, provides 3D compression and joint stabilization without restricting range of motion. It can help reduce stress on the shoulder joint while tissues calm down and healing progresses.
Can a Pinched Nerve in the Neck Cause Elbow Pain?
Yes. And this is where many people get confused.
If your elbow pain feels sharp, burning, or electric, and especially if it travels past the elbow into the forearm or hand, the source may not be your elbow or even your shoulder. It could be your neck.
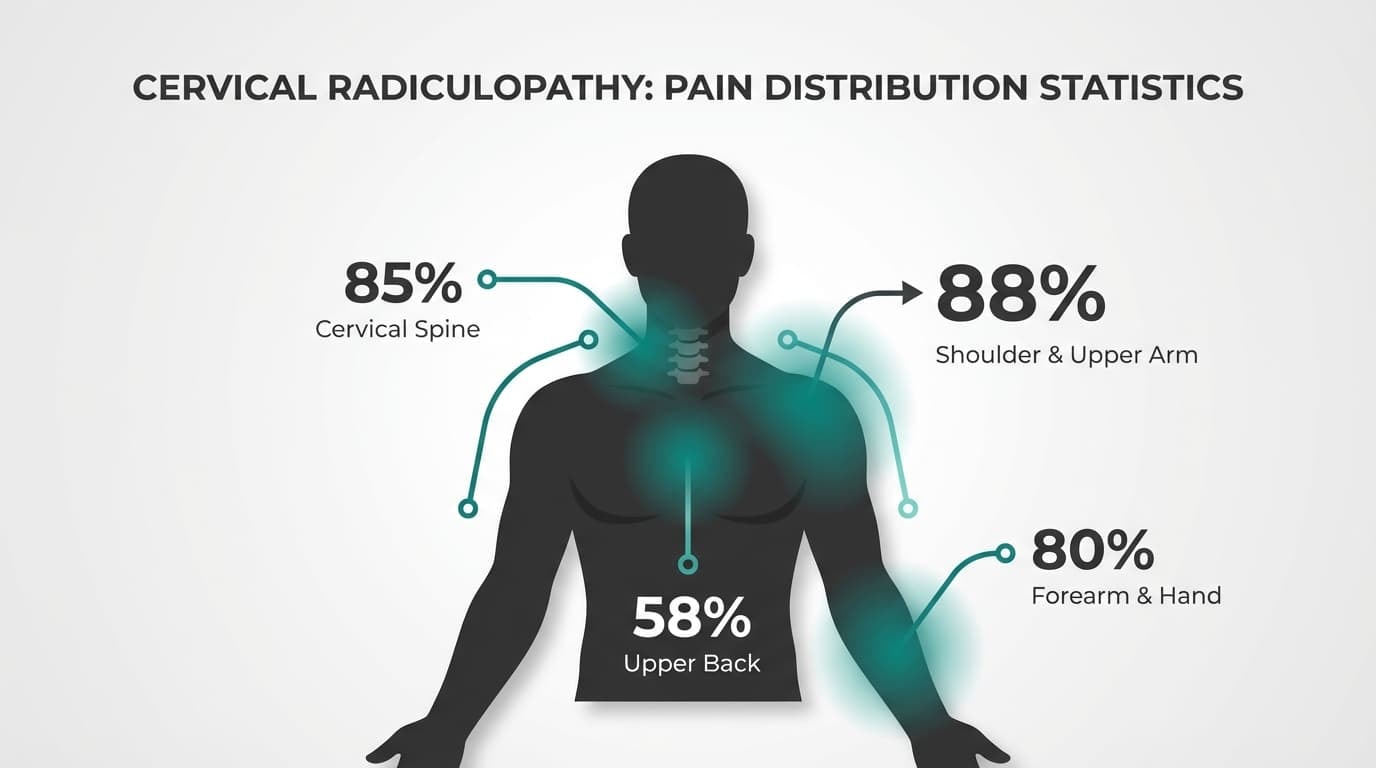
A 2025 scoping review analyzing 86 studies found that cervical radiculopathy produces arm pain in approximately 85% of cases and forearm pain in 58%. Neck and arm pain occurred together in 80% of cases, and neck, arm, and scapular pain in 58% of cases. Neck pain itself was reported in 88% of cases.
That matters.
When a nerve is irritated in your cervical spine, the pain does not stay neatly in one place. It can move down the arm, settle near the elbow, or even track into the hand. To the athlete or lifter, it feels like an elbow problem. Clinically, it may be a nerve pattern.
Differentiation between nerve root compression and mechanical shoulder pain relies on specific neurological markers:
-
Signal Quality: Nerve pain manifests as electric, lancinating, or burning sensations, distinct from the dull ache of tendinopathy.
-
Dermatomal Patterns: Symptoms follow specific nerve pathways—C6 compression typically affects the thumb side, while C8 affects the pinky side > Neck Positional triggers: Extension or rotation of the cervical spine (Spurling’s Maneuver) reproduces the distal arm pain.
If your symptoms shift with neck position, that is a strong clue. Elbow tendons do not change when you look left or right. Nerves do.
This is why proper screening matters. Treating a nerve problem, such as tennis elbow, delays recovery. Identifying the true source early makes everything simpler and safer.
When Elbow Pain Is Actually an Elbow Problem
Sometimes elbow pain is exactly what it sounds like. It is not referred from the shoulder. It is not coming from the neck. The elbow joint or surrounding tendons are the primary source.
Common true elbow conditions include:
-
Tennis elbow with pain on the outer bony part of the elbow
-
Golfer’s elbow with pain on the inner side
-
Olecranon bursitis with visible swelling at the back of the elbow
-
Early arthritis with stiffness and grinding during bending or straightening
A simple clue: you can point with one finger to where it hurts, and shoulder motion does not significantly change the pain.
It is also important to recognize red flags. A 2023 review of elbow assessment highlights urgent referral triggers, including fracture risk, unexplained swelling or masses, multi-joint inflammation, and suspected malignancy. If pain follows trauma with deformity, rapid swelling, fever, or if it feels systemic rather than mechanical, seek medical care promptly.
For typical overuse conditions, early management focuses on reducing load while staying active. This often includes:
-
Temporarily limiting repetitive gripping and heavy lifting
-
Gradual strengthening of the forearm muscles
-
Short, frequent breaks during desk or manual work
Some athletes also use temporary offloading support. An elbow strap or compression brace, such as the Anaconda Elbow Brace, can help reduce strain on irritated tendons during gripping or lifting tasks while recovery progresses.
The key is simple: treat the structure that is actually irritated, not just the place where you feel it.
Fast Self-Check: Is Your Elbow Pain Coming From the Shoulder or the Elbow?
If your elbow pain is frustrating and confusing, you are not alone. At Anaconda, we speak with athletes every day who are dealing with elbow and shoulder discomfort and trying to figure out what is actually causing thepain.
Before jumping into treatment options, you need clarity. This simple framework helps you understand whether your pain is likely coming from the shoulder, the elbow, or even nerve compression.
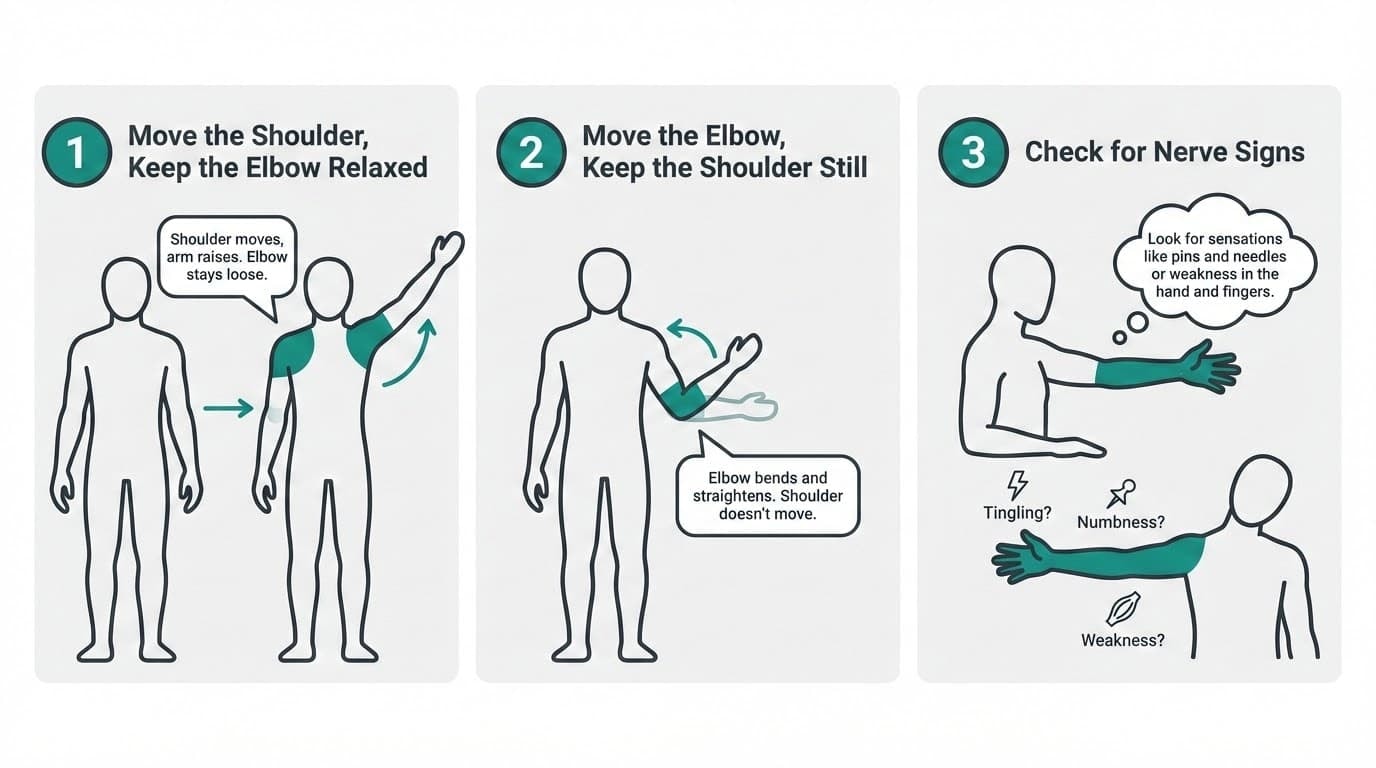
Step 1: Move the Shoulder, Keep the Elbow Relaxed
Let your elbow hang naturally. Now gently:
-
Lift your shoulder overhead
-
Rotate your arm outward
-
Reach behind your back
If these movements reproduce your familiar pain near the elbow, that suggests referred pain. In this case, the irritated structure may be in the shoulder, even though the elbow feels sore.
This is common with rotator cuff irritation or cervical radiculopathy, where nerve compression higher up in the neck causes pain further down the arm. The brain sometimes struggles to pinpoint exactly what is causing the pain, so discomfort can spread.
If shoulder motion clearly aggravates your elbow, it may be time to address shoulder mechanics rather than focusing only on the elbow itself.
Step 2: Move the Elbow, Keep the Shoulder Still
Now stabilize your shoulder and only move the elbow:
-
Bend and straighten it
-
Rotate your forearm
-
Lightly grip an object
If this directly triggers a sharp pain or a deep, dull ache at one specific spot, you may be dealing with primary elbow conditions.
Common examples include:
-
Lateral epicondylitis, often linked to repetitive motions and gripping
-
Medial epicondylitis, sometimes called golfer’s elbow
-
Overuse injuries affecting the forearm tendons
These elbow issues typically worsen with gripping, lifting, or repetitive strain. Unlike referred pain from the shoulder, you can usually point to the exact area causing pain.
Step 3: Check for Nerve Signs
Some common symptoms suggest nerve involvement rather than a tendon issue.
Ask yourself:
-
Does the pain travel past the elbow into the forearm or hand?
-
Do you feel tingling or burning?
-
Does neck movement change the symptoms?
If yes, cervical radiculopathy or nerve compression may be involved. This type of pain follows nerve pathways and often affects both the shoulder and elbow.
If weakness develops or pain persists and spreads, you should seek medical attention to avoid further complications.
When to Seek Medical Attention
While many cases improve with activity modification and strengthening of the surrounding muscles, certain signs require immediate medical attention:
-
Sudden severe shoulder or elbow pain after trauma
-
Rapid loss of strength
-
Swelling, deformity, or spreading redness
-
Pain accompanied by numbness that worsens
Ignoring red flags can lead to further complications. Early evaluation allows for a safer, more effective treatment plan.
What This Means for You
If your testing suggests shoulder involvement, the focus should be on shoulder stability, mobility, and reducing strain. If it feels like a true elbow condition, such as lateral or medial epicondylitis, load management and progressive strengthening are most important.
Treatment options may include:
-
Activity modification
-
Targeted strengthening
-
Bracing or support
-
Physical therapy
-
In some cases, steroid injections or corticosteroid injections under medical supervision
Surgery is rarely the first step. Even orthopaedic surgeons typically recommend conservative care before invasive treatment options.
The goal is not just reducing pain short term. It is about building a personalized treatment plan that addresses the actual cause of the pain, so you can return to training safely.
At Anaconda, we believe clarity comes first. Once you understand whether your elbow pain is shoulder-driven, nerve-related, or a true elbow issue, your next steps become much more straightforward.
Do You Need an MRI for Shoulder and Elbow Pain?
When pain shows up in your shoulder or elbow, it is completely normal to think an MRI is the next step. It feels clear. It feels definitive. But in many cases, imaging is not immediately necessary.
What Current Guidelines Suggest
2025 clinical practice guidelines published in JOSPT recommend against routine imaging for rotator cuff–related shoulder pain during the first 12 weeks unless certain red flags are present, such as:
-
Significant trauma
-
Progressive neurological changes
-
Concerning systemic symptoms
For many people, the first phase focuses on conservative care, like activity modification and structured rehabilitation.
Why Imaging Is Not Always the First Answer
Studies show that MRI scans can reveal structural shoulder changes in 20–30% of adults over 40 who report no shoulder pain.
This means not every finding on a scan is actually causing pain. Imaging results need to be interpreted alongside symptoms, strength, and movement quality.
When Shoulder-to-Elbow Pain Is Serious: Red Flags
Most shoulder and elbow pain is mechanical and improves with smart load management. However, there are situations where pain traveling from the shoulder to the elbow should not be ignored.
Clinical guidance from the 2025 JOSPT rotator cuff recommendations notes that red flags in shoulder assessment can include potential cardiovascular or visceral causes, particularly when pain presents alongside systemic symptoms.
Here are warning signs that require immediate medical attention:
-
Shoulder or arm pain with chest pressure, shortness of breath, sweating, nausea, or dizziness
-
Pain accompanied by fever or chills
-
A visibly deformed shoulder or elbow after trauma
-
Rapid swelling, unexplained lumps, or intense joint warmth
-
A history of cancer with new, unexplained shoulder or elbow pain
These symptoms should not be dismissed as routine training strain.
There are also neurological signs that deserve urgent evaluation:
-
Rapidly worsening weakness in the arm or hand
-
Progressive numbness that does not improve with position changes
-
Loss of coordination or repeated dropping of objects
At Anaconda, we support athletes through common shoulder and elbow challenges. But if symptoms suggest something beyond typical training stress, we always advise consulting a qualified medical professional immediately.
When something feels off in a serious way, get it checked.
How to Treat Shoulder-to-Elbow Pain Without Surgery
The good news is this: most shoulder-to-elbow pain improves without surgery. Whether the issue starts in the shoulder, involves mild nerve irritation, or includes certain elbow conditions, early conservative care is often enough to turn things around.
We see this pattern constantly with athletes managing training-related shoulder and elbow stress. The key is structured, progressive recovery.
Step 1: Reduce Aggravation, Not All Movement
First, reduce the load irritating the tissue. That may mean temporarily reducing:
-
Heavy overhead lifts
-
Repetitive pressing or throwing
-
Prolonged gripping or pulling movements
-
High-volume repetitive motions
Complete rest is rarely the answer. Controlled movement keeps the surrounding muscles active and prevents stiffness in the shoulder and elbow joints.
Step 2: Restore Strength and Control
A gradual rehab plan typically includes:
-
Rotator cuff and scapular stability work
-
Gentle mobility for the shoulder joint
-
Progressive loading for forearm muscles if elbow involvement is present
-
Postural and ergonomic adjustments
If nerve compression or cervical radiculopathy is contributing to symptoms, targeted neck mobility and nerve gliding techniques may be added under professional guidance.
Physical therapy can help build a personalized treatment plan that addresses both the source of pain and the mechanics that contributed to it.
Step 3: Support During Return to Training
As symptoms improve, many athletes begin a phased return to training rather than jumping straight back to full intensity.
During this stage, some athletes use structured compression supports to maintain alignment and reduce the risk of re-aggravation. A product like the Anaconda Shoulder Brace can provide 3D compression and joint stabilization while allowing a full range of motion. It is not a replacement for rehab, but it can help reduce strain on the shoulder during the transition back to heavier loads.
Step 4: Monitor Progress
Improvement usually happens gradually. Track:
-
Pain intensity week to week
-
How far does pain travel down the arm
-
Whether daily tasks feel easier
-
Whether the elbow stiffness or sharp pain is decreasing
If pain persists, worsens, or begins to involve increasing weakness, seek medical attention to avoid further complications.
Most shoulder and elbow issues respond well to early, consistent care. Surgery is typically reserved for significant structural damage or cases that fail to improve after months of structured treatment.
For most athletes, smart load management, strengthening, and patience are what actually restore performance.
What You Can Do This Week to Reduce Shoulder and Elbow Pain
If your shoulder and elbow pain are bothering you right now, focus on small, controlled adjustments. This week is about stabilizing the situation, not solving everything at once.
1. Change the Way You Train
Instead of stopping completely, modify intensity:
-
Lower the weight
-
Shortened range of motion
-
Reduce volume
-
Avoid movements that create sharp pain
You can still train around the issue. Just remove the specific stress that keeps triggering it.
2. Clean Up Daily Habits
Pain often lingers because of what happens outside the gym.
This week:
-
Keep your shoulders relaxed when sitting
-
Avoid hunching forward for long periods
-
Don’t rest your elbow directly on hard surfaces
-
Break up long desk sessions every 30–60 minutes
These small corrections reduce ongoing irritation without requiring major lifestyle changes.
3. Improve Warm-Ups
Before training:
-
Add 5–8 minutes of light shoulder and elbow activation
-
Do slow controlled arm circles
-
Add light resistance band work
-
Warm the joint before loading it
Cold, stiff tissue reacts poorly to sudden stress.
4. Train With Awareness
Pay attention to how the joint feels during movement:
-
Does pain spike suddenly?
-
Does it fade once warmed up?
-
Does it worsen after training?
Use that feedback to guide decisions the next day.
5. Consider Light Support
During early recovery, supportive compression can provide proprioceptive feedback. Some athletes find it helps them stay aware of joint positioning and avoid overloading irritated tissue.
Getting a Proper Diagnosis: What to Expect
If your pain has not improved or if the injury keeps returning, getting a proper evaluation is the next smart step. A clear diagnosis helps prevent guessing, unnecessary treatments, and further irritation.
At Anaconda, we always advise consulting a qualified healthcare professional for persistent shoulder and elbow pain, especially when an injury begins to affect strength or daily function.
The First Part Is Your Story
A clinician will start by asking questions like:
-
When did the injury begin?
-
Was it sudden or gradual?
-
What movements make it worse?
-
Do you play racquet sports or perform repetitive overhead training?
Many shoulder and elbow issues are commonly caused by repetitive loading. In racquet sports, for example, repetitive swings increase strain on the tendons and can increase the risk of overload injuries.
Understanding how your injury started often reveals the most common cause before any imaging is considered.
Physical Examination: Shoulder, Elbow, and Neck
A thorough exam usually includes checking:
-
Shoulder range of motion
-
Elbow stability
-
Strength of the surrounding muscles
-
Sensitivity along the tendons
-
Signs of limited mobility
-
Any signs of nerve irritation
Current clinical practice guidance emphasizes that providers should screen for cervical dysfunction and neurological symptoms when evaluating arm pain. That means your neck may also be assessed, even if you feel the pain closer to the elbow.
This matters because certain medical conditions, including cervical nerve irritation, can mimic shoulder and elbow problems.
What They Are Looking For
During the evaluation, clinicians try to determine:
-
Is this a tendon overload injury?
-
Is the rotator cuff involved?
-
Are the tendons inflamed or structurally compromised?
-
Is there nerve involvement?
-
Is this one of the more complex medical conditions affecting joint stability?
Tendon irritation is one of the most common causes of shoulder and elbow pain. However, instability, mechanical imbalance, or chronic overload can also contribute.
Imaging Is Not Always Step One
In many cases, imaging is not the immediate next step unless there are concerning findings. Structural changes in tendons can exist without severe symptoms, so exam findings are interpreted alongside your history.
Only when conservative care fails, or when there is suspicion of more significant injury, are surgical options considered. Most injuries respond well to non-surgical treatment plans.
What a Good Diagnosis Should Do
A proper evaluation should:
-
Identify the primary source of the injury
-
Rule out serious medical conditions
-
Outline realistic treatment options
-
Create a plan to provide relief
-
Reduce your risk of recurrence
The goal is not just to reduce pain short term. It is to understand why the injury occurred and how to prevent it from recurring.
When the diagnosis is clear, treatment becomes focused. And when treatment is focused, recovery is usually more efficient and far less frustrating.
Treatment Comparison Chart
Below is a simple side-by-side comparison to help you understand how treatment typically differs depending on whether your pain is primarily in the shoulder, neck, or elbow.
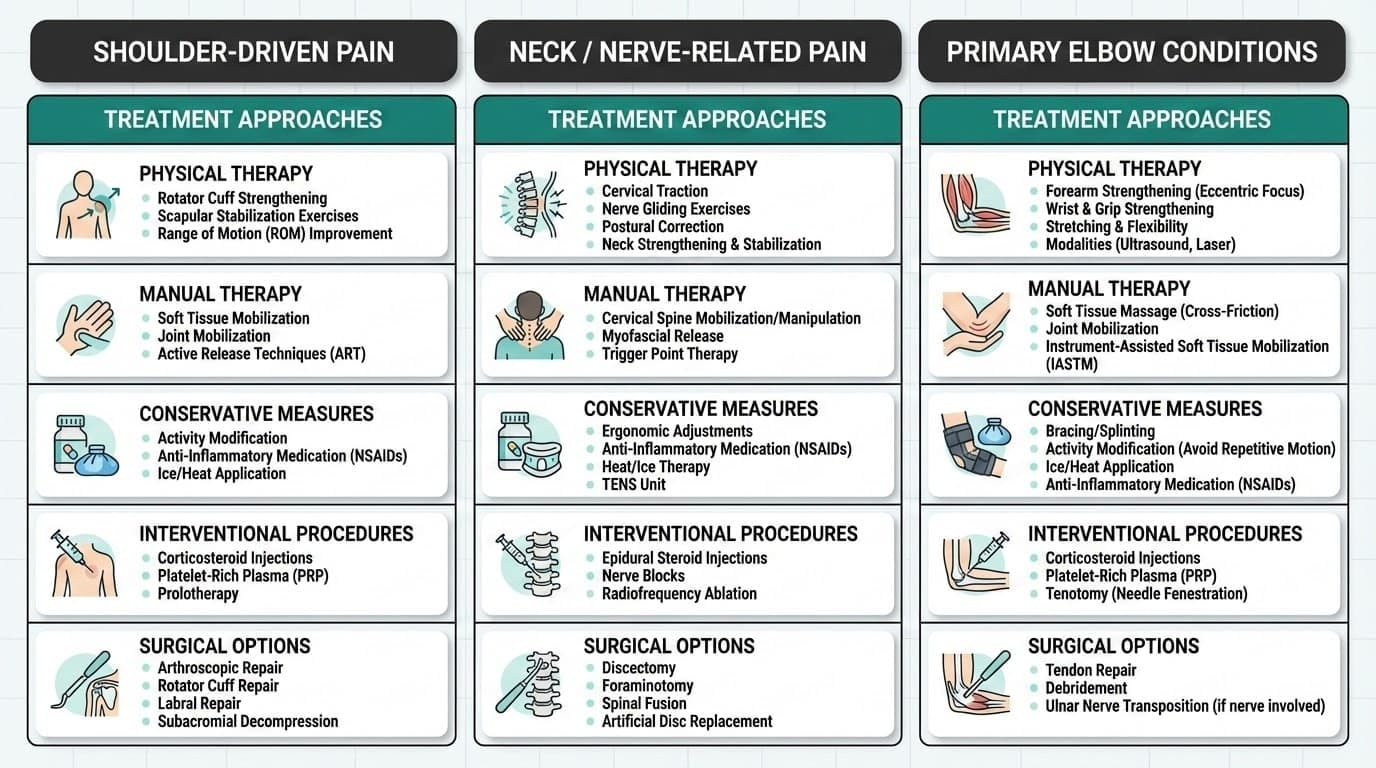
How to Use This Chart
-
If your pain changes when you move your shoulder, start in the shoulder column.
-
If symptoms travel past the elbow or change with neck position, look at the nerve column.
-
If pain is sharply localized at the elbow and aggravated by gripping or lifting, focus on elbow-specific care.
The goal is not to jump straight to advanced options. Most shoulder and elbow cases improve with structured, progressive treatment. Surgery is typically reserved for clear structural damage or cases that do not respond to consistent conservative management.
Clarity about the source makes treatment far more efficient.
Final Thoughts: Most Shoulder-to-Elbow Pain Improves With the Right Plan
If you are dealing with shoulder-to-elbow pain, take a breath. In most cases, this type of pain improves with early identification, smart load management, and consistent conservative care.
Whether the issue starts in the shoulder, involves mild nerve irritation, or relates to elbow overuse, surgery is rarely the first step. Intelligent training adjustments, progressive strengthening, and addressing movement mechanics usually make a meaningful difference over time.
The key is not ignoring pain, but responding to it strategically.
At Anaconda Fightwear, we believe training should feel strong, not uncertain. With the right plan, proper recovery, and structured support when needed, most shoulder-to-elbow pain can improve without stepping away from the sport you love.
FAQs
Quick answers to the most common shoulder-to-elbow pain questions we hear from athletes.
Can a rotator cuff problem really make just my elbow hurt?
Yes, a rotator cuff problem can sometimes make just your elbow hurt. Rotator cuff irritation often causes pain that travels down the upper arm and settles near the elbow. If shoulder movement triggers your elbow pain but pressing directly on the elbow does not, the source may be the shoulder. A proper assessment helps confirm whether it is a shoulder referral or a true elbow issue.
How long should I wait before seeing a doctor or physical therapist?
How long should you wait before seeing a doctor or physical therapist? If the pain is mild and improving within one to three weeks, careful self-management is reasonable. If pain is not improving, is limiting sleep or training, or lasts more than three to four weeks, it is time to get evaluated. Seek prompt care if you notice sudden weakness, deformity, chest symptoms, or spreading numbness.
Do I need an MRI to find out what’s causing my shoulder-to-elbow pain?
Do you need an MRI to find out what’s causing your shoulder-to-elbow pain? In most cases, no. Many shoulder and elbow problems can be identified through a detailed history and physical exam. Imaging is usually considered if symptoms do not improve after several weeks or if something more serious is suspected. Treatment often starts effectively without advanced scans.
Can bad posture or desk work cause shoulder and elbow pain together?
Yes, bad posture or desk work can cause shoulder and elbow pain together. Slouched sitting and unsupported arms increase strain on the neck, shoulder, and forearm. Over time, this can irritate shoulder tendons and overload elbow tissues. Small ergonomic adjustments and regular movement breaks can significantly reduce that stress.
Is shoulder-to-elbow pain always going to need surgery?
No, shoulder-to-elbow pain does not always need surgery. Most cases improve with load management, strengthening, and structured rehabilitation. Surgery is typically reserved for major tears, instability, or structural damage that does not improve with conservative care. The majority of athletes recover without operative treatment.













